
LOW BACK PAIN IN COMPETITIVE SWIMMERS AND ITS RELATIONSHIP WITH ANKLE DORSIFLEXION
DOLOR LUMBAR EN NADADORES DE COMPETICIÓN Y SU RELACIÓN CON LA FLEXIÓN DORSAL DE TOBILLO


Cristina Jiménez-Braganza, Germán Monterrubio-Fernández, Antonia Sáez-Díaz, Pedro V. Munuera-Martínez
LOW BACK PAIN IN COMPETITIVE SWIMMERS AND ITS RELATIONSHIP WITH ANKLE DORSIFLEXION
Cultura, Ciencia y Deporte, vol. 21, no. 67, 2026, 10.12800/ccd.v21i67.2376
Universidad Católica San Antonio de Murcia
Cristina Jiménez-Braganza a
Universidad de Sevilla, España
Germán Monterrubio-Fernández
Facultad Centro de Estudios Universitarios Cardenal Spínola CEU, España
Antonia Sáez-Díaz
Axioma Comunicaciones, España
Pedro V. Munuera-Martínez
Universidad de Sevilla, España
Received: 15 December 2024
Accepted: 29 June 2025
Abstract: Low back pain is a common musculoskeletal condition among competitive swimmers, and its occurrence may be related to biomechanical alterations in the lower limb. However, few studies have explored the influence of distal joint mobility on its development. A cross-sectional observational study was conducted with 157 federated swimmers (86 males and 71 females), divided into four categories: infant (14–15 years; n = 35), junior (16–20 years; n = 38), senior (≥21 years; n = 36), and master (>25 years; n = 48). The presence of low back pain was assessed using the NRPS-11 scale, and joint mobility was measured in the hip (flexion, extension, internal and external rotation), ankle dorsiflexion (with knee flexed and extended), and posterior muscle flexibility using the Seat and Reach test. A total of 66 swimmers (42.0%) reported low back discomfort. These swimmers showed significantly lower values in hip internal rotation and ankle dorsiflexion in both limbs (p < .05). Differences were consistent across all categories and swimming styles, with greater involvement observed in butterfly, backstroke, and master swimmers. An association was also found between reduced posterior flexibility (Seat and Reach test) and the presence of low back pain (p < .001). Limited joint mobility in the hip and ankle may be associated with low back pain in competitive swimmers. Systematic assessment of these factors may be useful for the prevention and management of muscle discomfort in this athletic population.
Keywords: Ankle, lower limb, muscle, swimming.
Resumen: El dolor lumbar es una alteración musculoesquelética frecuente en nadadores de competición, cuya aparición podría estar relacionada con alteraciones biomecánicas del miembro inferior. Sin embargo, pocos estudios han explorado la influencia de la movilidad articular distal en su desarrollo. Se realizó un estudio observacional transversal con 157 nadadores federados (86 hombres y 71 mujeres), distribuidos en cuatro categorías: infantil (14–15 años; n = 35), junior (16–20 años; n = 38), absoluta (≥21 años; n = 36) y máster (>25 años; n = 48). Se evaluó la presencia de molestias lumbares mediante la escala NRPS-11 y se midió la movilidad articular de cadera (flexión, extensión, rotación interna y externa), la flexión dorsal de tobillo (con rodilla flexionada y extendida) y la flexibilidad de la musculatura posterior mediante el test de Seat and Reach. Un total de 66 nadadores (42,0 %) reportaron molestias lumbares. Estos presentaron valores significativamente menores en la rotación interna de cadera y en la flexión dorsal de tobillo en ambas extremidades (p < .05). Las diferencias fueron consistentes en todas las categorías y estilos, con mayor afectación en mariposistas, espaldistas y nadadores máster. También se observó asociación entre la flexibilidad posterior reducida (test de Seat and Reach) y la presencia de dolor lumbar (p < .001). La movilidad articular limitada en cadera y tobillo podría estar asociada al dolor lumbar en nadadores de competición. Su evaluación sistemática puede resultar útil para la prevención y el abordaje de molestias musculares en este grupo deportivo.
Palabras clave: Miembro inferior, músculos, natación, tobillo.
Introduction
Lower-limb injuries are common in sport. These injuries are multifactorial and may be influenced by environmental, biomechanical, and anatomical factors, among others. Historically, research has focused on the exact site of pain without considering more distal structures (Niemuth, 2007). Swimming is a sport in which performance depends on mechanical efficiency. The aquatic environment creates resistance to forward motion, limiting the effects of force application. In this context, flexibility may provide a mechanical advantage by enabling a greater range of motion and allowing more productive force application (Nichols, 2015). Swimming is associated with a relatively low incidence of injuries compared with other sports. However, its cyclical and repetitive nature increases injury risk, with the shoulder being the most frequently affected region, followed by the lumbar spine and the knee (Matsuura et al., 2019). Low back pain is a highly prevalent musculoskeletal condition among athletes. It has been estimated to affect up to 94% of athletes at some point during their sporting careers (Miyamori et al., 2023) and occurs in approximately 22–47% of swimmers. It is characterized by increased tension in the hip extensors, weakness in the abdominal and hip flexor muscles, and lumbar spine instability (Miyamori et al., 2023). Different swimming strokes require the lumbar spine to remain in hyperextension in order to maintain a more hydrodynamic position, which may increase injury risk (Nichols, 2015). Previous studies have shown that abnormal lower-limb function may contribute to increased low back pain (Sadler et al., 2017). Within the pelvic complex between the hip and the ankle, several joint segments may influence the lumbar region and consequently affect locomotion, highlighting the importance of biomechanical research. Limb-length discrepancy may lead to changes in trunk, pelvic, and lower-limb kinematics and muscle activation (Rahimi et al., 2020). Reduced lumbar and hip range of motion may also be associated with pelvic tilt, contributing to lumbar overload (Dehcheshmeh et al., 2024). Although swimming has been widely recommended as a therapeutic modality for individuals with chronic low back pain (CLBP) due to its low joint impact and beneficial effects on mobility, the available evidence mainly refers to the general population rather than elite athletes. In this regard, the qualitative study by Oakes et al. (2025) suggests that swimming can act as an effective self-management strategy in people with CLBP, providing pain relief, functional improvement, and emotional well-being. However, in the context of high performance, biomechanical demands, accumulated training loads, and sustained body positions during practice may produce opposite effects, generating muscular overload and restrictions in joint mobility. Therefore, the profile of the competitive swimmer should be addressed differently from general therapeutic recommendations.
Swimming is a sport in which the winner is determined by thousandths of a second, and professionals continually seek new ways to improve performance (Demi̇rkan et al., 2021). In swimmers’ leg movements, including underwater undulatory swimming during starts and turns, previous research has shown a relationship between trunk movements and foot angulation (Tanaka et al., 2022). This relationship contributes to maintaining proper body alignment and increasing swimming speed. This may be because a greater ankle range of motion during kicking could influence the generation of greater propulsive force (Tanaka et al., 2022).
To date, no studies have been found in the literature reporting whether lower-limb alterations such as limited ankle dorsiflexion (DF) are associated with low back pain in competitive swimmers. Due to this lack of information, the aim of this study was to examine the relationship between ankle dorsiflexion in competitive swimmers and the presence of low back pain.
Materials and Methods
This was a cross-sectional observational study involving competitive swimmers from different swimming clubs in Seville (Spain), conducted between February 2022 and August 2023. All adult participants, as well as the parents or legal guardians of underage swimmers, provided written informed consent to participate voluntarily in the study. The study was approved by the Ethics Committee of the University of Seville.
As inclusion criteria, participants were required to belong to one of the official competitive swimming categories (youth, junior, senior, or master) according to their age group and competitive level at the time of assessment. The minimum age for participation was 14 years. Athletes were required to train an average minimum of 10 km per week and to be specialized in at least one swimming stroke.
Swimmers practicing other aquatic disciplines, as well as those with any degree of disability or a history of fracture or surgery affecting the lower limb, were excluded from the study.
Participants
A total of 157 competitive swimmers (86 men and 71 women) voluntarily participated in this study: 35 swimmers in the youth category (INF) aged 14–15 years, 38 in the junior category (JUN) aged 16–20 years, 36 in the senior category (ABS) aged 21 years or older, and 48 in the master category (MAST) aged 25 years or older. In total, 314 lower limbs were analyzed.
Instruments
Information on the swimmers’ general characteristics was collected, including age, sex, and body mass index (BMI). Sport-specific variables related to swimming practice were also recorded, such as weekly swimming distance, main swimming stroke, and years of swimming experience. Subsequently, a physical examination was performed in which the following variables were assessed: presence of lumbar muscle discomfort, hip rotation (internal and external), hip flexion and extension, the Sit-and-Reach test, and ankle mobility. Data were collected immediately after the swimmers’ in-water training sessions. For the measurements, a two-arm goniometer was used to assess hip flexion and extension, an inclinometer was used to measure internal and external hip rotation, and a sit-and-reach box with a millimeter-scale ruler on its surface was used to perform the Sit-and-Reach test (Merino et al., 2011).
Procedure
Lumbar discomfort was defined as pain that appeared spontaneously during swimming, without any previous traumatic event. To assess the level of pain or discomfort, the Numeric Rating Pain Score–11 (NRPS-11) was used, where a value of zero corresponds to the absence of pain and values from 1 to 10 indicate the presence of pain of different intensities (Breivik et al., 2008). This scale was administered individually to each swimmer immediately after the aquatic training session, in a controlled environment and without external interference. Each participant was instructed to indicate the level of lumbar discomfort perceived during swimming, considering only spontaneous pain not related to any previous trauma, fall, or impact. The presence of low back pain was considered when participants reported a value equal to or greater than 1 on the NRPS-11 scale and localized the discomfort in the region between the lower costal margin and the gluteal fold, following standardized clinical criteria.
Variables related to low back pain were measured, including hip range of motion in flexion–extension and internal and external rotation (Rahimi et al., 2020), as well as the Sit-and-Reach test (SRT), which provided quantifiable information on posterior chain flexibility (Carrasco et al., 2013). In addition, ankle dorsiflexion was quantified to determine whether swimmers with low back pain presented a reduced ankle range of motion.
Although several validated clinical tests exist to assess lumbar flexibility more specifically, such as the modified Schober test or trunk inclinometry, the Sit-and-Reach test (SR) was selected exclusively for several methodological and contextual reasons. First, the SR test has demonstrated good criterion validity for estimating the extensibility of the hamstring muscles and the lumbosacral region in physically active populations (Carrasco et al., 2013; López-Miñarro et al., 2015). Moreover, it allows for the combined assessment of key structures of the posterior kinetic chain involved in swimming mechanics, such as the hamstrings, spinal erectors, and thoracolumbar fascia.
Additionally, the operational context of the study (conducted after training sessions in sports clubs) required a non-invasive, quick, and standardized assessment method that could be applied to a large number of participants without interfering with their usual sporting routine. The SR test meets these requirements and has been widely used in previous studies involving swimmers and other athletes as a reliable tool to detect global functional restrictions of the posterior chain (Merino et al., 2011; Nichols, 2015). Its selection was therefore justified based on feasibility, methodological consistency, and practical applicability in real sporting environments.
Regarding ankle mobility, a two-arm goniometer was used, as described in standard clinical reference manuals (Norkin & White, 2019; Taboadela, 2013). Ankle dorsiflexion was measured in two different positions to identify the potential involvement of the biarticular gastrocnemius muscle in limiting joint range of motion:
-
With the knee extended, to assess combined ankle mobility with the gastrocnemius under stretch.
-
With the knee flexed (approximately 90°), to isolate ankle joint mobility by reducing the action of the gastrocnemius.
In both cases, the axis of the goniometer was positioned over the lateral malleolus, aligning one arm with the midline of the leg and the other with the longitudinal axis of the fifth metatarsal. The maximum passive dorsiflexion range achieved was recorded, ensuring the absence of compensatory movements in other joints and standardizing the initial position.
Hip flexion was measured with the athlete in the supine position on the examination table. The center of the two-arm goniometer was placed over the center of the hip joint, with the proximal arm aligned with the lateral aspect of the femur and the distal arm aligned with the lateral aspect of the pelvis. To measure hip extension, the athlete was placed in the prone position, aligning the goniometer with the same anatomical landmarks. Both internal and external hip rotation were measured using an inclinometer. The athlete was seated at the edge of the examination table with the knees flexed at 90°. The inclinometer was placed on the anterior tibial tuberosity, using the anterior midline of the leg as a reference. The foot was moved outward to measure internal rotation and inward to measure external rotation. During all mobility assessments, the hip was required to remain stable, avoiding compensatory movements that could distort the measurements (Norkin & White, 2019).
In addition, the Sit-and-Reach (SR) test was applied, as it is widely used in the scientific literature to assess global flexibility of the posterior trunk and lower-limb musculature (Merino et al., 2011; Carrasco et al., 2013; López-Miñarro et al., 2015). This test was used to explore potential muscular tightness within the posterior chain that could be associated with functional shortening patterns. To assess lumbar flexibility using the SR test, participants were seated on the floor with the knees fully extended and the feet in contact with the measurement box. The ankles were maintained in a neutral position, avoiding plantar flexion. Participants were instructed to perform maximal trunk flexion by sliding both hands along the millimeter scale of the box, and the maximum distance reached was recorded without bouncing (López-Miñarro et al., 2015).
To determine the presence of gastrocnemius tightness, differences between ankle dorsiflexion measured with the knee flexed and extended were analyzed. The axis of the two-arm goniometer was placed over the lateral malleolus, with one arm aligned along the midline of the leg and the other along the longitudinal axis of the fifth metatarsal (Taboadela, 2013).
Finally, the joint mobility data obtained from the participating swimmers were compared with reference values for joint range of motion (ROM) in healthy individuals reported in the international scientific literature (Norkin & White, 2019; Taboadela, 2013; Van Ost, 2010).
Statistical Analysis
For the descriptive analysis, absolute frequency (N), relative frequency (%), mean values, standard deviation (SD), and the 25th, 50th, and 75th percentiles (interquartile range) were calculated.
The Shapiro–Wilk test (for groups with N ≤ 50) or the Kolmogorov–Smirnov test (for groups with N > 50) was used to assess whether the data followed a normal distribution.
When the data met the assumptions of normality, parametric tests were applied for comparisons or correlations; otherwise, non-parametric tests were used.
To determine differences between groups, the independent-samples t-test was used for variables with a normal distribution, and the Mann–Whitney U test was applied for non-normally distributed variables. Spearman’s correlation coefficient was used to analyze the relationships between hip rotations, hip flexion–extension, and ankle dorsiflexion (with the knee extended and flexed). Statistical analyses were performed using IBM SPSS Statistics version 27.
Results
A total of 157 competitive swimmers participated in this study, of whom 86 were men (54.8%) and 71 were women (45.2%), resulting in the analysis of a total of 314 lower limbs. The sample was distributed by competitive category as follows: 35 youth swimmers (22.3%), 38 junior swimmers (24.2%), 36 senior swimmers (22.9%), and 48 master swimmers (30.6%). According to the main competitive swimming stroke, the sample consisted of 26 butterfly swimmers (16.6%), 32 backstroke swimmers (20.4%), 31 breaststroke swimmers (19.7%), 64 freestyle swimmers (40.8%), and 4 individual medley swimmers (2.5%). At the time of data collection, the mean weekly training volume was 26.3 ± 13.9 km, and the mean swimming experience was 12.8 ± 8.6 years. The number of swimmers who reported lumbar discomfort during swimming was 66 (42.0%).
This section presents exclusively the results that reached statistical significance following the analyses performed. Additional data that did not show statistically significant differences but are considered of complementary interest have been included as supplementary material available at the end of the article.
Table 1 shows the relationship between hip rotation, hip flexion–extension, and low back pain. Swimmers in our sample exhibited lower values of internal hip rotation compared with external rotation. As shown, swimmers with low back pain presented lower internal rotation values (30.2 ± 4.7, right side; 30.4 ± 4.6, left side). For hip external rotation, the results differed between limbs, and therefore no conclusive findings were obtained. Regarding hip flexion–extension, no statistically significant results were observed.
Comparison Between Hip Rotation, Hip Flexion–extension, and Low Back Pain
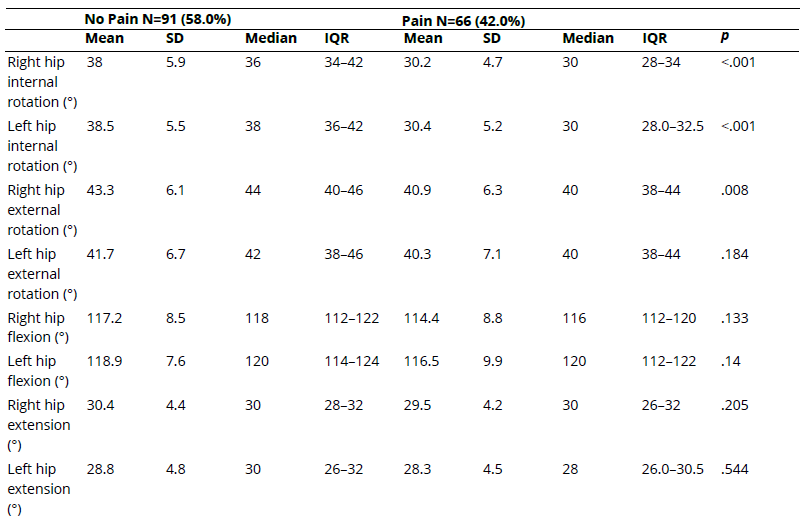
Note SD: standard deviation; IQR: interquartile range; (°) = degrees.
In Table 2, the results analyzing the differences between swimmers with and without low back pain are presented. Statistically significant differences were observed in several joint variables. Internal were higher in swimmers without pain (34.8° ± 4.7 and 36.1° ± 4.5) compared with those reporting lumbar discomfort (29.6° ± 4.5 and 29.4° ± 4.5). A similar pattern was observed in women, in whom mean values decreased from 40.3° ± 5.7 and 40.2° ± 5.6 in the no-pain group to 32.0° ± 4.8 and 33.0° ± 6.1 in the pain group. These differences were statistically significant (p < .001).
Regarding hip flexion, a statistically significant difference was found only on the right side in women (p = .042), with swimmers reporting pain showing a reduced range of motion (116.7° ± 6.8) compared with the no-pain group (120.8° ± 7.5). No statistically significant differences were observed for the remaining hip flexion measurements.
Significant differences were also detected in ankle dorsiflexion with the knee extended, both on the right and left sides. In both limbs and in both sexes, swimmers with low back pain exhibited lower ranges of motion (7.5° ± 3.6 in men and women) compared with those without pain (8.9° ± 3.8 for the right side and 9.1° ± 3.8 for the left side), with p-values of 0.009 and 0.006, respectively.
Comparison Between Hip Mobility, Ankle Dorsiflexion, and Low Back Pain by Sex
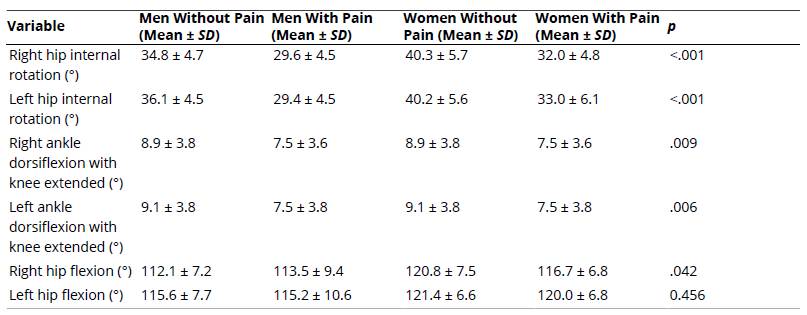
Note SD: standard deviation; (°) = degrees.
In Table 3, joint mobility values are analyzed in swimmers who reported low back pain according to their competitive category, where statistically significant differences were observed in several variables. Internal hip rotation, both right and left, showed significant differences between categories (p < .001), with master-category swimmers presenting the lowest values (27.0° ± 4.2 and 26.9° ± 4.1, respectively), in contrast to the highest values observed in the junior category (33.4° ± 3.7 and 32.7° ± 3.7, respectively).
Regarding right hip external rotation, significant differences were also found (p = 0.044), with master swimmers again showing the lowest values (35.6° ± 6.3) compared with junior swimmers (44.9° ± 5.8). However, left hip external rotation did not show statistically significant differences (p = .163), despite a tendency toward lower values in the master category.
With respect to hip flexion, significant differences between categories were identified for both the right and left sides (p = .007 and p = .025, respectively). The highest left hip flexion values were recorded in the senior category (120.9° ± 4.6), whereas the lowest values were observed in the master category (113.8° ± 14.0), which may reflect a reduction in joint mobility associated with age and sporting career progression.
Comparison Between Hip Mobility and Low Back Pain According to Competitive Category
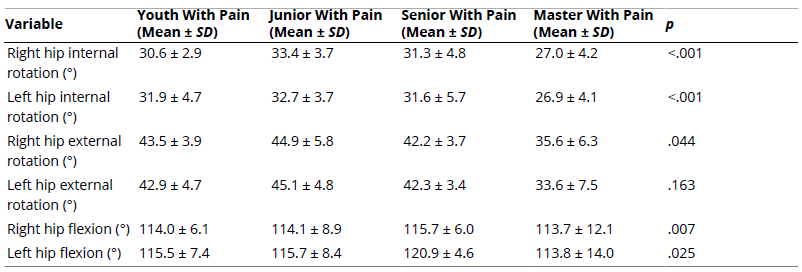
Note SD: standard deviation; (°) = degrees.
In Table 4, analyses conducted according to the main swimming stroke also revealed significant differences in joint mobility among swimmers with low back pain. Internal hip rotation, both right and left, showed statistically significant variations between swimming strokes (p < .001 in both cases). Backstroke swimmers presented the greatest ranges of motion (31.8° ± 3.6 and 32.4° ± 4.2), whereas freestyle swimmers exhibited the lowest values (29.4° ± 5.8 and 29.4° ± 6.1).
Regarding left hip extension, a statistically significant difference was found between swimming strokes (p = .045), with the lowest values observed in butterfly swimmers (25.0° ± 1.7) and the highest values in backstroke swimmers (29.3° ± 4.3). No statistically significant differences were found for right hip extension (p = .481).
Comparison Between Hip Mobility and Low Back Pain According to the Main Swimming Stroke
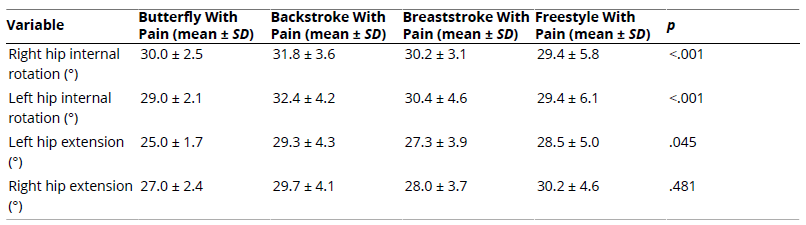
Note SD: standard deviation; (°) = degrees.
In Table 5, the comparison between ankle dorsiflexion and low back pain is presented. The results show statistically significant differences in ankle dorsiflexion (DF) between swimmers with and without low back pain, both with the knee extended and with the knee flexed. In all measurements, values were consistently lower in the group reporting low back pain.
Under the knee-extended condition, swimmers without pain showed a mean ankle dorsiflexion of 8.9° ± 3.8 in the right ankle and 9.1° ± 3.8 in the left ankle, compared with 7.5° ± 3.6 and 7.5° ± 3.8, respectively, in the pain group. These differences were statistically significant (p = .009 and p = .006).
Similarly, with the knee flexed, swimmers without pain exhibited greater ranges of motion (17.1° ± 4.7 and 17.6° ± 4.7) than those reporting discomfort (15.2° ± 4.6 and 15.2° ± 5.0 for the right and left sides, respectively), with p-values also reaching statistical significance (p = .010 and p = .006). These findings suggest an association between reduced ankle dorsiflexion mobility and the presence of low back pain.
Comparison Between Ankle Dorsiflexion and Low Back Pain
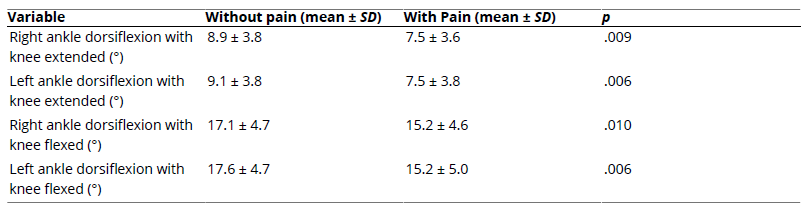
Note SD: standard deviation; DF: dorsiflexion; (°) = degrees.
In Table 6, the relationship between ankle dorsiflexion, both with the knee flexed and extended, and hip rotation and flexion–extension variables are presented. The results show an association between these variables; however, the strength of the relationship is weak.
Relationship Between Hip Rotation, Hip Flexion–extension, and Ankle Dorsiflexion With the Knee Flexed and Extended
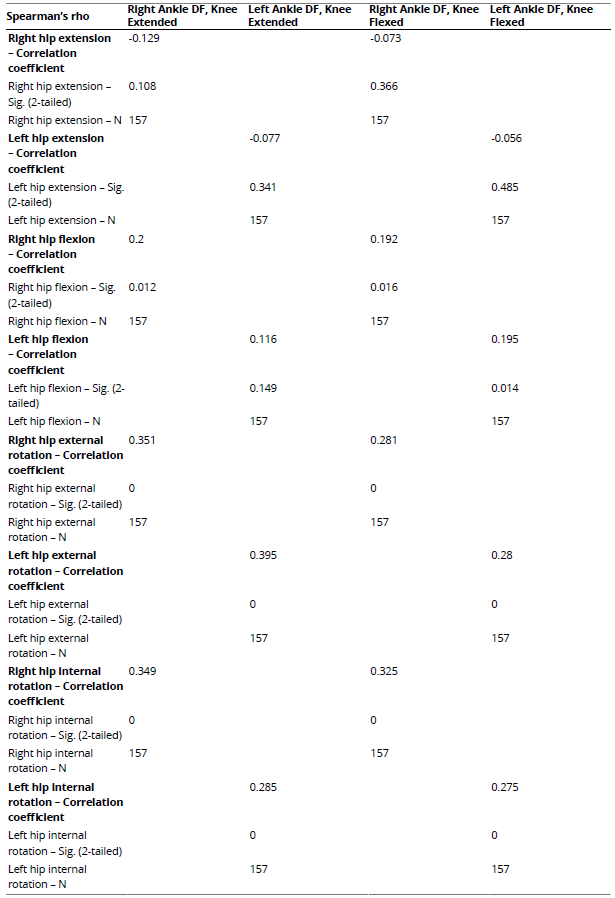
Note *p<0.05; **p<0.001
In Table 7, the comparison between low back pain and the Sit-and-Reach test is presented. Of the total sample (157 swimmers), 77 (49.0%) showed low values on the Sit-and-Reach test. The results revealed statistically significant differences, with p < .05.
Comparison Between Low Back Pain and the Sit-and-Reach Test

Discussion
The aim of this study was to analyze low back pain in competitive swimmers and its relationship with limitations in ankle mobility. To the best of our knowledge, this is the first study to report data on the relationship between low back pain and foot-related variables in competitive swimmers.
Lower-limb asymmetries may influence athletic performance, and one possible cause is the functional adaptations required by the specific sport practiced (Phukan et al., 2021). These adaptations, together with reduced flexibility, may lead to muscular imbalances and the adoption of incorrect postures during swimming (Sanders et al., 2011). Although the relationship between lower-limb asymmetries and performance in swimmers remains unclear due to the scarcity of previous research, some authors suggest that swimming does not promote asymmetries because both body hemispheres are trained equally, even though swimming strokes themselves are not perfectly symmetrical (Palomino-Martín et al., 2015). In contrast, our results indicate the presence of differences in lower-limb range of motion (ROM) between both extremities, suggesting the existence of asymmetries within the sample.
With regard to flexibility, excessive muscle shortening reduces the interosseous space and limits joint range of motion. Achieving an appropriate muscular balance is therefore essential to ensure optimal joint mobility (Serra et al., 2017). Swimming requires a large ankle ROM to achieve efficient propulsion. When ankle mobility is reduced, hydrodynamic resistance increases and propulsion efficiency decreases (Noto-Bell et al., 2019). Previous studies have shown that a 5° increase in ankle dorsiflexion contributes to a significant increase in propulsive forces (Shen et al., 2022). Another key variable influencing swimming performance is hip rotation (Demi̇rkan et al., 2021). In swimmers with low back pain in our study, a clear muscular imbalance between internal and external hip rotation was observed.
Low back pain has been reported in 22-47% of swimmers. A previous study identified a high degree of lumbar disc degeneration in swimmers compared with a control group (Nichols, 2015). Although Kaneoka et al. (2007) stated that determining the exact cause of low back pain is complex, it should be considered that increased lumbar tension may not be solely attributable to the sustained hyperextension required during swimming, but also to rotational movements (Nichols, 2015). Khodaee et al. (2016) reinforced this argument, proposing that trunk rotation during breathing may fatigue spinal stabilizers. In addition, swimmers must constantly adjust their center of buoyancy to maintain an optimal hydrodynamic position, requiring coordinated activation of the abdominal muscles and spinal extensors to prevent the lower limbs from sinking (Hsu et al., 2024).
Kitamura et al. (2020) suggested that hip flexor musculature may reduce lumbar extension provided that it is not excessively tense. Although swimmers are often characterized by greater joint laxity, the ROM of their hip rotators tends to be reduced. This observation is consistent with our findings, as swimmers with low back pain exhibited decreased hip rotational movements. St-Pierre et al. (2022) demonstrated that internal hip rotation and hip extension increase intracapsular tension up to five times more than hip flexion movements. These authors further suggested that discomfort associated with internal hip rotation may originate from musculoskeletal alterations in the lumbar region. From a technical perspective, swimming requires the lower limbs to be positioned in lumbar extension, with the hip in internal rotation and adduction.
Regarding the relationship between low back pain and hip rotation, Miñambres-Martín et al. (2022) reported that athletes with low back pain exhibit reduced hip extension, which is often compensated by increased hip rotational movements. They also noted that internal hip rotation is diminished in individuals with low back pain. In our study, swimmers with low back pain showed reduced hip extension compared with asymptomatic swimmers, although these differences were not statistically significant. However, in agreement with previous studies, swimmers with low back pain exhibited significantly reduced internal hip rotation. Cejudo et al. (2020) emphasized that limitations in hip rotation are clinically relevant because they lead to compensatory movements in the lumbosacral region. These authors also highlighted the importance of the balance between internal and external hip rotation, noting that a difference greater than 5-10° increases the incidence of low back pain. In our study, swimmers in younger competitive categories with low back pain showed differences greater than 10° between internal and external hip rotation.
When examining the relationship between trunk mobility and ankle dorsiflexion (DF), previous research has suggested an association between kick efficiency and trunk mobility in swimmers. Faster swimmers appear to increase displacement by enhancing joint ROM rather than increasing kick frequency. However, a lack of evidence persists regarding the influence of trunk mobility on foot kinematics (Kaneoka et al., 2007). Pabón Carrasco et al. (2019) reported that limited ankle DF may predispose individuals to low back pain, as reduced ankle ROM is associated with altered pelvic alignment and biomechanical asymmetries between limbs. Rahimi et al. (2020) observed that individuals with low back pain exhibit reduced pelvic rotation and decreased ankle motion in the sagittal plane, suggesting that any dysfunction within the hip-ankle complex may influence the onset of low back pain.
Reduced ankle DF ROM leads to lumbopelvic adaptations and an increased torsional moment in the lower limbs, thereby increasing the likelihood of low back pain (Rao et al., 2024). Limited ankle DF restricts tibial advancement over the talus, reducing knee flexion capacity and promoting compensatory hip movements, often positioning the hip in adduction (Rabin et al., 2016). In swimming, the hip must be maintained in sustained adduction and internal rotation, and as shown in our results, swimmers with low back pain exhibited reduced internal hip rotation (Palmer et al., 2015). These authors also highlighted the importance of ankle position in relation to posterior chain flexibility, indicating that resistance to ankle DF reflects increased tissue tension when attempting to achieve greater joint positions, particularly involving the hamstrings and hip musculature.
Although Kaneda et al. (2023) suggested that competitive swimmers exhibit greater foot flexibility than other athletes due to joint laxity, our findings indicate that competitive swimmers with low back pain present a reduced ankle ROM. Several studies have shown that restrictions in ankle dorsiflexion alter lower-limb and lumbopelvic biomechanics. Pabón Carrasco et al. (2019) demonstrated that limited ankle DF in individuals with pronated feet and low back pain affects pelvic alignment and induces biomechanical asymmetries between limbs, potentially leading to compensatory pelvic adaptations that increase lumbar stress. In our study, swimmers with low back pain showed significantly lower ankle DF values, both with the knee extended and flexed, compared with asymptomatic swimmers, supporting this hypothesis.
Rahimi et al. (2020) also reported reduced pelvic rotation and sagittal-plane ankle ROM in individuals with low back pain. This combination of distal stiffness and pelvic restriction forces intermediate structures, such as the hip joint and lumbar spine, to assume a greater functional ROM, increasing the risk of overuse or overload. In our sample, this compensatory mechanism manifested as reduced internal hip rotation in swimmers with lumbar discomfort, particularly in strokes requiring greater body control, such as butterfly and backstroke. Rao et al. (2012) further noted that reduced ankle DF angles during gait increase torsional moments in the lumbopelvic region, leading to muscular adaptations, imbalanced activation, and greater fatigue of trunk stabilizers-an effect particularly relevant in cyclical sports such as swimming.
Our findings are consistent with this framework, as we observed a statistically significant association between limited ankle DF and the presence of lumbar discomfort across all age categories. This suggests a direct functional involvement of distal mobility in lumbopelvic stability. Palmer et al. (2015) also demonstrated that increased resistance during ankle dorsiflexion is associated with shortening of the hamstrings and triceps surae, reducing mechanical efficiency and increasing overload risk during movements involving hip extension and internal rotation, such as underwater undulatory swimming or butterfly kicking. In line with this, butterfly and backstroke swimmers with low back pain in our study exhibited significantly reduced hip extension and internal rotation, potentially reflecting a pattern of rigidity and functional overload.
Taken together, these biomechanical findings support our results, indicating that limited ankle mobility and hip joint imbalances are associated with the development of lumbar discomfort during swimming. Functional assessment of these variables should therefore be integrated into injury prevention strategies for competitive swimmers.
Conclusions
The results obtained in our research on competitive swimmers indicate an association between reduced hip rotation and limited ankle dorsiflexion. Competitive swimmers who reported muscular discomfort during swimming showed greater shortening of the triceps surae musculature together with reduced ankle dorsiflexion, compared with swimmers who did not report discomfort during training. Limitation of ankle dorsiflexion is related to hip rotation, and as hip rotation decreases in these athletes, the prevalence of low back pain increases.
Study Limitations
This study presents several limitations that should be considered when interpreting the results. First, the cross-sectional design prevents the establishment of causal relationships between the analyzed variables. In addition, the assessment of low back pain was based on self-reported questionnaires, which may introduce recall bias or subjective perception. Although objective tests were used to evaluate ankle mobility, a detailed kinematic analysis of the swimming technical gesture was not included, which could provide additional insight into the underlying mechanisms. Furthermore, the sample was limited to competitive swimmers from a specific geographic region, which may restrict the generalizability of the findings to other populations or competitive levels. Future longitudinal studies with larger samples could help to confirm and expand upon these results.
Practical Implications
The results of this study have relevant implications for training and injury prevention in high-performance swimming. The identification of reduced ankle dorsiflexion as a potential factor associated with low back pain highlights the importance of incorporating periodic functional assessments into swimmers’ monitoring programs. In addition, the implementation of specific preventive strategies is recommended, such as joint mobility exercises, muscle stretching before and after training sessions, and posterior chain flexibility work, particularly in athletes with a history of lumbar discomfort. These measures may help reduce the risk of compensatory overloads during the technical gesture and improve the mechanical efficiency of swimming.
Ethics Committee Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Research Ethics Committee of the University of Seville (internal code 250522). Date: 01/12/2022.
Conflict of Interest Statement
The authors declare that there is no conflict of interest.
Funding
This research did not receive funding because it is the author’s own work.
Authors’ Contribution
Conceptualization: Cristina Jiménez-Braganza; Pedro V. Munuera-Martinez; Methodology: Cristina Jiménez-Braganza; Pedro V. Munuera-Martinez; Software: Pedro V. Munuera-Martinez; Antonia Sáez-Díaz; Validation: Cristina Jiménez-Braganza; Pedro V. Munuera-Martinez; Antonia Sáez-Díaz; Germán Monterrubio-Fernández; Formal Analysis: Pedro V. Munuera-Martinez; Antonia Sáez-Díaz; Investigation: Cristina Jiménez-Braganza; Resources: Cristina Jiménez-Braganza; Pedro V. Munuera-Martinez; Antonia Sáez-Díaz; Germán Monterrubio-Fernández; Data Curation: Pedro V. Munuera-Martinez; Writing – Original: Cristina Jiménez-Braganza; Writing – Review & Editing: Pedro V. Munuera-Martinez; Antonia Sáez-Díaz; Germán Monterrubio-Fernández; Visualization: Cristina Jiménez-Braganza; Germán Monterrubio-Fernández; Supervision: Pedro V. Munuera-Martinez; Project Administration: Pedro V. Munuera-Martinez. All authors have read and agreed with the published version of the manuscript.
Data Availability Statement
The data supporting the findings of this study are available on request from the corresponding author. The data is not publicly available due to ethical or privacy restrictions.
Referencias
Breivik, H., Borchgrevink, P. C., Allen, S. M., Rosseland, L. A., Romundstad, L., Breivik Hals, E. K., Kvarstein, G., & Stubhaug, A. (2008). Assessment of pain. British Journal of Anaesthesia, 101(1), 17-24. https://doi.org/10.1093/bja/aen103
Carrasco, M., Sanz-Arribas, I., Martínez-de-Haro, V., Cid-Yagüe, L., & Martínez-González-Moro, I. (2013). ¿El test ‘Sit and Reach’ mide la flexibilidad? Un estudio de casos. Revista Internacional de Medicina y Ciencias de la Actividad Fisica y del Deporte, 13(52), 749-770. https://repositorio.uam.es/server/api/core/bitstreams/8d00f664-19a3-4ba4-8bb9-015e35b459f1/content
Cejudo, A., Moreno-Alcaraz, V. J., Izzo, R., Santonja-Medina, F., & Sainz De Baranda, P. (2020). External and total hip rotation ranges of motion predispose to low back pain in elite Spanish inline hockey players. International Journal of Environmental Research and Public Health, 17(13), 4858. https://doi.org/10.3390/ijerph17134858
Dehcheshmeh, F. G., Nourbakhsh, M. R., Amini, Z., Bazrgari, B., & Arab, A. M. (2024). Kinematic analysis of pelvic and lower limb joints during stand-to-sit movement in individuals with chronic low back pain: A cross-sectional study. The Archives of Bone & Joint Surgery, 12(8), 587–596. https://doi.org/10.22038/ABJS.2024.76840.3551
Demi̇rkan, E., Özkadi, T., Can, S., & Alagöz, İ. (2021). Does ankle plantar and dorsiflexion affect fifty-meter swimming time in swimmers? Turkish Journal of Sport and Exercise, 23(3), 353-358. https://izlik.org/JA62EL66BL
Hsu, C., Krabak, B., Cunningham, B., & Borg-Stein, J. (2024). Swimming anatomy and lower back injuries in competitive swimmers: A narrative review. Sports Health: A Multidisciplinary Approach, 16(6), 971-981. https://doi.org/10.1177/19417381231225213
Kaneda, K., Maeda, N., Ikuta, Y., Tashiro, T., Tsutsumi, S., Arima, S., Sasadai, J., Suzuki, Y., Morikawa, M., Komiya, M., Adachi, N., & Urabe, Y. (2023). The features of foot morphology and intrinsic foot muscle property in adolescent swimmers: An ultrasound-based study. Journal of Human Kinetics, 88, 95–103. https://doi.org/10.5114/jhk/163148
Kaneoka, K., Shimizu, K., Hangai, M., Okuwaki, T., Mamizuka, N., Sakane, M., & Ochiai, N. (2007). Lumbar intervertebral disk degeneration in elite competitive swimmers: A case control study. American Journal of Sports Medicine, 35(8), 1341-1345. https://doi.org/10.1177/0363546507300259
Kitamura, G., Tateuchi, H., & Ichihashi, N. (2020). Greater lumbar extension during dolphin kick and psoas major tightness in swimmers with low back pain. Journal of Sport Rehabilitation, 29(6), 716–722. https://doi.org/10.1123/JSR.2018-0262
Khodaee, M., Edelman, G. T., Spittler, J., Wilber, R., Krabak, B. J., Solomon D., Riewald, S., Kendig, A., Borgelt, L. M., Riederer, M., Puzovic, V., & Rodeo, S. (2016). Medical care for swimmers. Sports Med – Open, 2, e27. https://doi.org/10.1186/s40798-016-0051-2
López-Miñarro, P. Á., Vaquero-Cristóbal, R., Muyor, J. M., & Espejo-Antúnez, L. (2015). Criterion-related validity of sit-and-reach test as a measure of hamstring extensibility in older women. Nutricion Hospitalaria, 32(1), 312–317. https://doi.org/10.3305/nh.2015.32.1.8999
Matsuura, Y., Hangai, M., Koizumi, K., Ueno, K., Hirai, N., Akuzawa, H., & Kaneoka, K. (2019). Injury trend analysis in the Japan national swim team from 2002 to 2016: Effect of the lumbar injury prevention project. BMJ Open Sport and Exercise Medicine, 5(1), 1–8. https://doi.org/10.1136/bmjsem-2019-000615
Merino, R., Mayorga, D., & Fernandez, E. (2011). Validity of sit-and-reach test for the assessment of hamstring muscle extensibility in junior level triathletes. Trances: Revista de Transmisión del Conocimiento Educativo y de la Salud, 3(3), 415–434. https://fb39c223-56a9-4ed3-91f4-073579bde094.filesusr.com/ugd/fa6be1_9e33c37a2088433c9e7d0374f6a3f7ab.pdf
Miñambres-Martín, D., Martín-Casas, P., López-de-Uralde-Villanueva, I., Fernández-de-las-Peñas, C., Valera-Calero, J. A., & Plaza-Manzano, G. (2022). Physical function in amateur athletes with lumbar disc herniation and chronic low back pain: A case-control study. International Journal of Environmental Research and Public Health, 19(6), 3743. https://doi.org/10.3390/ijerph19063743
Miyamori, T., Saito, T., Aoyagi, M., Nozu, S., Masui, Y., Ishihara, Y., Shimasaki, Y., & Yoshimura, M. (2023). Differences in the elastic modulus of the lumbar muscles between female athletes with and without low back pain. Clinical Biomechanics, 105, 105968–105968. https://doi.org/10.1016/j.clinbiomech.2023.105968
Nichols, A. W. (2015). Medical care of the aquatics athlete. Current Sports Medicine Reports, 14(5), 389–396. https://doi.org/10.1249/JSR.0000000000000194
Niemuth, P. E. (2007). The role of hip muscle weakness in lower extremity athletic injuries. International SportMed Journal, 8(4), 179–192. https://hdl.handle.net/10520/EJC48623
Norkin, C. C., & White, D. J. (2019). Manual de goniometría: Evaluación de la movilidad articular. Paidotribo.
Noto-Bell, L., Vogel, B. N., & Senn, D. E. (2019). Effects of post–isometric relaxation on ankle plantarflexion and timed flutter kick in pediatric competitive swimmers. Journal of Osteopathic Medicine, 119(9), 569–577. https://doi.org/10.7556/jaoa.2019.100
Oakes, H., Stephensen, D., Mills, H., & De Vivo, M. (2025). Learning to swim with back pain: a qualitative study of swimmers with chronic low back pain. International Journal of Qualitative Studies on Health and Well-being, 20(1), 2474357. https://doi.org/10.1080/17482631.2025.2474357
Pabón Carrasco, M., Gago Reyes, F., Fernández Seguín, L., Munuera Martínez, P. V., Palomo Toucedo, I. C., & Castro Méndez, A. (2019). Limited ankle dorsiflexion in subjects with pronated feet and low back pain. Fisioterapia, 41(2), 89–94. https://doi.org/10.1016/j.ft.2019.02.005
Palmer, T. B., Akehi, K., Thiele, R. M., Smith, D. B., Warren, A. J., & Thompson, B. J. (2015). Dorsiflexion, plantar-flexion, and neutral ankle positions during passive resistance assessments of the posterior hip and thigh muscles. Journal of Athletic Training, 50(5), 467–474. https://doi.org/10.4085/1062-6050-49.6.04
Palomino-Martín, A., González-Martel, V., Quiroga-Escudero, M. E., & Ortega-Santana, F. (2015). Efectos del entrenamiento de natación sobre la asimetría corporal en adolescentes. International Journal of Morphology, 33(2), 507–513. https://doi.org/10.4067/S0717-95022015000200016
Phukan, M. I., Thapa, R. K., Kumar, G., Bishop, C., Chaabene, H., & Ramirez-Campillo, R. (2021). Inter-limb jump asymmetries and their association with sport-specific performance in young male and female swimmers. International Journal of Environmental Research and Public Health, 18(14), 7324. https://doi.org/10.3390/ijerph18147324
Rabin, A., Portnoy, S., & Kozol, Z. (2016). The association of ankle dorsiflexion range of motion with hip and knee kinematics during the lateral step-down test. Journal of Orthopaedic & Sports Physical Therapy, 46(11), 1002–1009. https://doi.org/10.2519/jospt.2016.6621
Rahimi, A., Arab, A. M., Nourbakhsh, M. R., Hosseini, S. M., & Forghany, S. (2020). Lower limb kinematics in individuals with chronic low back pain during walking. Journal of Electromyography and Kinesiology, 51, 102404. https://doi.org/10.1016/j.jelekin.2020.102404
Rao, S., Riskowski, J. L., & Hannan, M. T. (2012). Musculoskeletal conditions of the foot and ankle: Assessments and treatment options. Best Practice and Research Clinical Rheumatology, 26(3), 345–368. https://doi.org/10.1016/j.berh.2012.05.009
Rao, Y., Yang, N., Gao, T., Zhang, S., Shi, H., Lu, Y., Ren, S., & Huang, H. (2024). Effects of peak ankle dorsiflexion angle on lower extremity biomechanics and pelvic motion during walking and jogging. Frontiers in Neurology, 14, 1269061. https://doi.org/10.3389/fneur.2023.1269061
Sadler, S. G., Spink, M. J., Ho, A., De Jonge, X. J., & Chuter, V. H. (2017). Restriction in lateral bending range of motion, lumbar lordosis, and hamstring flexibility predicts the development of low back pain: A systematic review of prospective cohort studies. BMC Musculoskeletal Disorders, 18(1), 179. https://doi.org/10.1186/s12891-017-1534-0
Sanders, R. H., Thow, J., & Fairweather, M. (2011). Asymmetries in swimming: Where do they come from? Journal of Swimming Research, 18, 1–11. https://cdn.ymaws.com/swimmingcoach.org/resource/resmgr/swimresearch/coaching-app-sanders-vol18.pdf
Serra, N., Carvalho, D. D., & Fernandes, R. J. (2017). The importance of agonistic, antagonist and synergistic muscles coordination on swimming dry land training. Trends in Sport Sciences, 3(24), 101–104. https://doi.org/10.23829/TSS.2017.24.3-1
Shen, Y., Fu, Y., Ge, Y., & Wen, Y. (2022). The effect of ankle flexibility on the relationship between knee isokinetic strength and the speed of underwater dolphin kicks in male competitive swimmers. Isokinetics and Exercise Science, 30(1), 61–68. https://doi.org/10.3233/IES-200255
St-Pierre, M.-O., Lavoie, F.-A., Brismée, J.-M., Hoffmann, M., Begon, M., Bertrand-Grenier, A., & Sobczak, S. (2022). Intracapsular pressures in the flexion-abduction-external rotation and flexion-adduction-internal rotation tests and their comparison with classic hip range of motion: A cadaveric assessment. Clinical Biomechanics, 91, 105526. https://doi.org/10.1016/j.clinbiomech.2021.105526
Taboadela, C. H. (2013). Goniometria. Una herramienta para la evaluación de las incapacidades laborales (1.Ed.). Asociart ART.
Tanaka, T., Hashizume, S., Sato, T., & Isaka, T. (2022). Competitive-level differences in trunk and foot kinematics of underwater undulatory swimming. International Journal of Environmental Research and Public Health, 19(7), 3998. https://doi.org/10.3390/ijerph19073998
Van Ost, L. (2010). Cram session in goniometry: A handbook for students and clinicians. Slack Incorporated.
Author notes
a Correspondence: Cristina Jimenez-Braganza, cjimenez8@us.es
Additional information
Short title: Low Back Pain in Competitive Swimmers
How to cite this article: Jiménez-Braganza, C., Monterrubio-Fernández, G., Sáez-Díaz, A., & Munuera-Martínez, P. V. (2026). Low back pain in competitive swimmers and its relationship with ankle dorsiflexion. Cultura, Ciencia y Deporte, 21(67), 2376. https://doi.org/10.12800/ccd.v21i67.2376






