




Acute effects of different facemasks during High Intensity Interval Training in trained women. A randomized crossover pilot study


Carmen Daniela Quero-Calero, Daniel López-Plaza, Oriol Abellán-Aynés, Luis Andreu-Caravaca, Pedro Manonelles Marqueta, José Manuel García-De Frutos
Acute effects of different facemasks during High Intensity Interval Training in trained women. A randomized crossover pilot study
Cultura, Ciencia y Deporte, vol. 17, no. 54, 2022
Universidad Católica San Antonio de Murcia
Carmen Daniela Quero-Calero
International Chair of Sports Medicine, Catholic University of Murcia, Spain
Faculty of Sport, Catholic University of Murcia, Spain
Daniel López-Plaza * dlplaza@ucam.edu
International Chair of Sports Medicine, Catholic University of Murcia, Spain
Oriol Abellán-Aynés
International Chair of Sports Medicine, Catholic University of Murcia, Spain
Faculty of Sport, Catholic University of Murcia, Spain
Luis Andreu-Caravaca
International Chair of Sports Medicine, Catholic University of Murcia, Spain
Faculty of Sport, Catholic University of Murcia, Spain
Pedro Manonelles Marqueta
International Chair of Sports Medicine, Catholic University of Murcia, Spain
José Manuel García-De Frutos
Faculty of Sport, Catholic University of Murcia, Spain
Received: 29 April 2022
Accepted: 04 july 2022
Abstract: The aim of the present investigation was to analyze the acute effect of different facemasks on physiological, perceptual and performance parameters in trained young women during a High Intensity Interval Training (HIIT) on cycle ergometer. Fifteen subjects participated in the study. Heart rate variability, muscle oxygen saturation, lactate concentration and comfort parameters were measured under 3 conditions: no facemask, surgical and FFP2 facemask. The use of facemasks had no effect on any variable related to oxygen saturation, heart rate variability and cycling power during the HIIT protocol. Only lactate concentration revealed significantly lower values in the No mask condition compared to FFP2 3 min after HIIT (p = .038). Regarding the overall perception and comfort, participants reported greater discomfort when wearing the FFP2 mask compared to the No mask condition (p<.05). On the contrary, the analysis of heart rate variability, revealed significant differences (p<.001) in the Pre compared to the Post exercise for all conditions. The use of surgical or FFP2 facemask during HIIT training does not affect performance during strenuous exercise while perceived comfort appears to be lower with FFP2 masks in physically trained women.
Keywords: facemask, interval training, exercise, Covid-19, women.
Resumen: El objetivo de esta investigación fue analizar los efectos agudos de diferentes tipos de mascarillas sobre los parámetros fisiológicos y comodidad en mujeres entrenadas durante un entrenamiento interválico de alta intensidad (HIIT) en cicloergómetro. Quince sujetos fueron examinados, obteniendo la variabilidad de la frecuencia cardíaca, la saturación de oxígeno muscular, la concentración de lactato y los parámetros de confort bajo 3 condiciones: sin mascarilla, mascarilla quirúrgica y mascarilla FFP2. El uso de mascarillas no tuvo efecto sobre la saturación de oxígeno, la variabilidad de la frecuencia cardíaca y la potencia de pedalada durante el ejercicio. Sólo la concentración de lactato reveló valores significativamente más bajos Sin mascarilla que con FFP2 3 min después del HIIT (p = .038). En cuanto a la percepción y comodidad, los participantes identificaron una mayor incomodidad con el uso de FFP2 en comparación con la ausencia de ésta (p<.05). Por el contrario, el análisis de la variabilidad de la frecuencia cardíaca, reveló diferencias significativas (p<.001) en el ejercicio Pre- comparado con el Post- en todas las condiciones. El uso de mascarilla quirúrgica o FFP2 durante el entrenamiento HIIT no afecta al rendimiento, mientras que la comodidad percibida parece ser menor con las mascarillas FFP2 en mujeres entrenadas.
Palabras clave: mascarilla, entrenamiento interválico, ejercicio, Covid-19, mujer.
Introduction
One of the most common ways of SARS-CoV-2 spreading, cause of Covid-19, is by close contact through respiratory droplets. There is growing evidence that the use of facemasks prevents its contagion and transmission (Chu et al., 2020; Leung et al., 2020; Wang et al., 2020), since they are considered a worldwide useful mitigation strategy during the pandemic (Esposito et al., 2020). Typically, Surgical and Filtering Face Piece (FFP2) are recommended facemasks, but they meet different filtration requirements. The FFP2 facemask filters small airborne particles and offers fewer facial seal leaks, making it more effective in reducing viral infections than surgical facemasks (Smith et al., 2016).
High Interval Intensity Training (HIIT) method has become popular not only for athletes to improve performance in endurance (Billat, 2001; Laursen & Jenkins, 2002) but also for sedentary and active individuals (Gibala et al., 2012; Kemi & Wisløff, 2010). HIIT can be defined as repeated bouts of high intensity exercise, from a maximal lactate steady state (MLSS) or point of respiratory compensation (CPR) to a total supramaximal exercise intensity, interspersed with recovery periods (Koichiro Azuma & Matsumoto, 2016). With exercises at these intensities oxygen systems are exposed to maximum stress, which provides the most effective stimulus to increase maximum oxygen consumption (VO2max) (Buchheit & Laursen, 2013; Seiler & Sjursen, 2004). Therefore, the ability to perform that type of vigorous physical activity with some type of facemask could be a problem (Chandrasekaran & Fernandes, 2020) as physiological impact during vigorous physical activity is unknown (Bailey et al., 2015). Moreover, some physiological effects associated with the use of facemasks such as decreasing muscle metabolism or increasing cardiorespiratory and mental stress have been recently reported and might have and influence on discomfort during exercise (Chandrasekaran & Fernandes, 2020).
Recent studies have successfully used infrared spectroscopy to monitor muscle oxygen saturation (SmO2) during intense activities such as HIIT (Olcina et al., 2019; Paquette et al., 2020). The predominant metabolism during intense and strenuous exercise is the anaerobic, which needs a large amount of oxygen (O2) for an efficient lactic acid conversion (Jacobson et al., 2019). An increase in arterial carbon dioxide (CO2) may occur due to the constant breathing of previously exhaled air (closed cycle), resulting in an acidic environment, increasing lactate levels, and consequently a rapid onset of fatigue in the athlete. All this will result in a worse hemoglobin saturation and the appearance of a hypoxic environment of all vital organs (Chandrasekaran & Fernandes, 2020; Jacobson et al., 2019). In addition, to quantify autonomic cardiac activity (Thayer et al., 2010) or exercise-induced adaptations (Barbosa et al., 2014) some methods such as heart rate variability (HRV) have been widely used.
Currently, results on whether the use of facial facemask impairs the performance of the exercise has been analyzed by incremental cycling test (Epstein et al., 2021; Fikenzer et al., 2020; Shaw et al., 2020) and on a treadmill (Wong et al., 2020) but the results with strenuous physical activity tests such as the HIIT method are unknown. Moreover, physiological differences between males and females may be a factor to consider because females have smaller lungs and rib cages (Dominelli et al., 2019) and consequently smaller conducting airways while males have a higher minute ventilation who may have a greater increase in work of breathing while wearing a facemask during intense efforts (Hopkins et al., 2021).
The effect of HIIT exercise using different facemasks has never been investigated taking into consideration gender differences. Thus, the main aim of the current study was to analyze the effect of not wearing a facemask, wearing a surgical facemask or wearing a FFP2 facemask on different physiological, perceptual and performance responses in trained young women during a HIIT protocol on a cycle ergometer.
Methods
Participants
Sixteen physically-trained females with a regular participation (3 times a week) in high intensity endurance activities voluntarily participated in this investigation. During the study one “experimental death” occurred resulting in a final sample of 15 participants (23.67 ± 3.04 years of age, 58.33 ± 6.93 kg of body mass and 164.97 ± 8.98 cm of height).
Facemasks
In the protocol study two types of facemasks were used: FFP2 (Qh Medicine, Jiangsu, China) and surgical (Cmc Medical Device, Málaga, Spain) with bacterial filtration capacity >99%. Both facemasks are commercially available to hospitals and pharmacies complying with all the sanitary guarantees.
Experimental design
A randomized crossover design was performed to analyze the possible different effects of diverse facial facemask types during a high intensity protocol. The facemask-type based groups were stablished as: a) No mask, b) Surgical: and c) FFP2. Each participant was randomly assigned a facemask-type group order by using a computerized randomization scheme. The inclusion criteria were: a) being female; b) being physically active in endurance activities (at least 6 hours per week); and c) between 18 and 30 years of age. The exclusion criteria included: a) presenting any injury or cardiorespiratory disease; and/or b) taking medication that could interfere with the results of the study. All subjects participated in the experiment only when they were during follicular phase.
All participants were informed about the study and were asked to provide written informed consent before participating in the study, which had been previously approved by the Ethics Committee of the Catholic University of Murcia (Spain) following current legislation (CE012103).
The participants were asked to come to the laboratory rested and having performed no vigorous exercise in the preceding 48 h. The anthropometric parameters analyzed included height (cm), measured by a stadiometer (Seca 222, Hamburg, Germany) and weight (kg), which was recorded with a Seca 634 scale (Hamburg, Germany).
Every participant attended the laboratory four times, at the same time of the day on four different days using the same procedures and materials. The first session consisted in a familiarization with the protocol whereas the other three were counterbalanced HIIT (High Intensity Interval Training) sessions, one with surgical facemask, (SM), one with FFP2 facemask (FM) and one with no facemask (NM). Figure 1 shows a schematic diagram during a session of the study protocol.
Outcomes
Experimental protocol
Each session lasted about 30 min. The temperature (22º) and relative humidity (53%) of the laboratory remained constant during all the trials. The same warm-up was performed in all sessions, consisting of 5 min of continuous pedaling on the cycle ergometer, at 100 W, with 1 min rest before starting the protocol. An electronically controlled cycle ergometer (Technogym Bike, Med Technogym SpA, Cesena, Italy) with a workload mode independent of pedaling frequency was used. In the first session the participants self-selected their exercise intensity in response to a prescription of “effort maximum interval and session” and was maintained along the other sessions. Participants were instructed to remain seated on the cycle ergometer during the test. In total, 8 high intensity intervals of 30 s were performed, respectively, analyzing the maximum power (Pmax) and average power (Pmean) in watts (W) every 5 s during the HIIT intervals.
Heart rate variability
The HRV measurements were carried out at resting in a supine position for 10 minutes, being analyzed only the last 5 min to ensure that a resting heart rate was achieved. The analysis of only 5 min was performed in accordance with the HRV task force (Camm et al., 1996).
HRV estimations were performed with a pulse sensor Polar H7 (Kempele, Finland) to assess beat-to-beat data during the evaluations. The examination of HRV variables was done through the product Kubios HRV 3.0. This product was additionally used to apply filters for artifact correction if necessary. The time- and frequency-domain as well as Poincare plot variables were obtained. The time-domain factors investigated were the mean heart rate (HR), mean R-R interval time in ms (RR), the standard deviation of consecutive R-R intervals (SDNN), the root mean square of successive differences of consecutive R-R intervals in ms (RMSSD) and the relative value of consecutive intervals that differ by more than 50 ms (pNN50). At last, Poincare plot factors such as the standard deviation of instantaneous beat-to-beat interval variability (SD1) and the continuous long-term R-R interval variability (SD2) were determined. Stress score (SS) was calculated by 1000 x 1/SD2, and the sympathetic/parasympathetic ratio (S/PS) was determined through SS/SD1.
Blood Lactate
To obtain the blood lactate concentration, a portable lactate analyzer (Lactate Scout system, RedMed, Warsaw, Poland) was used. Lactate concentration was measured according to the principle of enzymatic determination by photometric reflection. For that purpose, a capillary blood drop sample was taken under safety standards from the index finger of the subject's right hand. In order to obtain a correct and hygienic collection, nursing material such as latex gloves, sterile gauze, lancets and 98º alcohol were used.
To observe lactate levels as a function of the test, a total of three measurements were performed: 1) baseline level (previous to the protocol and warm-up); 2) post-test after 1 min; and 3) post-test after 3 min.
Muscle Oxygen Saturation
Muscle oxygen saturation was measured by a MOXY monitor (Fortiori Design LLC). The device uses four wavelengths of Near-Infrared Spectroscopy (NIR) light at 680, 720, 760, and 800 nm (Schmitz, 2015) to identify changes in total tissue hemo- (+myo-) globin (tHb). Before testing, a moxy device was placed only on the anterolateral part of the right thigh (right vastus lateralis of the quadriceps femoris), at 1/3 distance between the patella and greater trochanter, parallel to the longitudinal femur axis and above the upper patella border. Data acquisition was obtained from the sensors internal memory from the Moxy PC software.
Perceived effort and comfort of physical activity
To measure perceived exertion and comfort levels during physical activity two measurements were used, the rating of perceived exertion (RPE) (Borg, 1998) and one scale for subjective comfort with the use of different facemasks (Li et al., 2005).
Rating of perceived exertion (RPE): during the 30-second rest period of each protocol interval participants were required to assign a value (1 to 10) according to their levels of perceived exertion, with a value of 10 being the maximum perceived effort.
Rating of perceived discomfort: at the end of the cycloergometer protocol of each session, participants were asked about some markers of discomfort with the use of the face facemask (humidity, heat, breathing resistance, itchiness, tightness, saltiness, feeling unfit, odor, fatigue, and overall discomfort), ranging from 0 (not at all, comfortable) to 10 (strongly discomfort).
The Physical Activity Enjoyment Scale (PACES) adapted to Spanish (Moreno et al., 2008) was used at the end of each session of the study protocol. Responses were collected on a Likert-type scale whose score ranges ranged from 1 (strongly disagree) to 5 (strongly agree). The final PACES score was obtained according to the procedures from Motl et al., (2001).
Statistical analysis
Data collection, treatment, and analysis were performed using the SPSS for Windows statistical package (version 20.0; SPSS, Inc., Chicago, IL, USA). Measures of homogeneity and spread were reported as mean and standard deviation (s). The hypotheses of homogeneity of variance and normality of the distribution were analyzed using the Levene’s test and Kolmogorov–Smirnov test, respectively. The comparisons of facemask groups means were performed using repeated measures analysis of variance (ANOVA) test with three levels (no facemask, Surgical and FFP2) when statistical tests revealed no violations of the assumptions of normality and homogeneity. To identify the significance between groups when ANOVA revealed significant differences, post hoc Bonferroni tests with corrections were conducted. Friedsman test was used when normality supposition of data was rejected, whereas if any significant difference between groups were identified, post hoc Wilcoxon signed-rank tests with Bonferroni corrections were performed. The level of significance was set as . < .05 and partial eta squared (η2p) was calculated as a measure of effect size, considering small size when between .01 and .06, moderate when between .06 and .13, and large when the effect was > .13.
Results
The results of the oxygen saturation and HRV parameters before and after a HIIT protocol depending on the type of facemask are presented in Table 1. No significant differences were observed in any oxygen-related variable. Conversely, the analysis of heart rate variability revealed significant differences (p < .001) in all facemask conditions as a consequence of HIIT effect in all variables investigated, observing large effect sizes higher than .74 in all cases.
Oxygen saturation and heart rate variability parameters before and after a HIIT protocol wearing different face masks (No, Surgical and FFP2 mask)
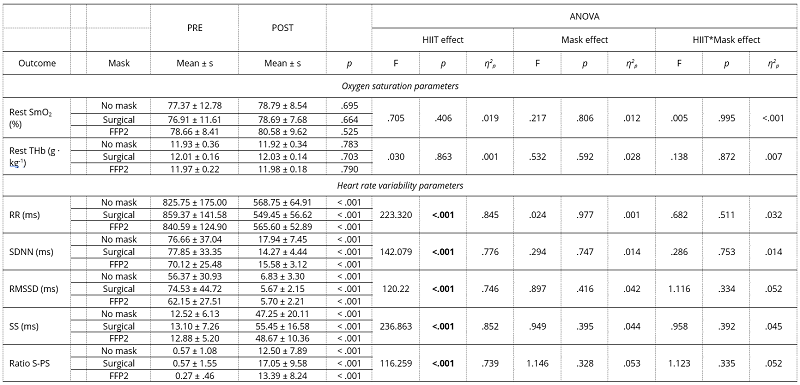
HIIT: high intensity interval training; SmO2: muscle oxygen concentration; THb: total tissue hemo- (+myo-) globin; RR: R-R interval time; SDNN: standard deviation of consecutive R-R intervals; RMSSD; root mean square of successive differences of consecutive R-R intervals; SS: stress score
In addition, Figure 1 shows the changes in mean values of cycling Power, SmO2 and RPE for each of the HIIT intervals when wearing different facemasks. Mean values of blood lactate concentration and HR are presented in Figure 2. Significant lower lactate concentration in the No facemask condition compared to FFP2 was detected 3 min after the HIIT (p = .038).
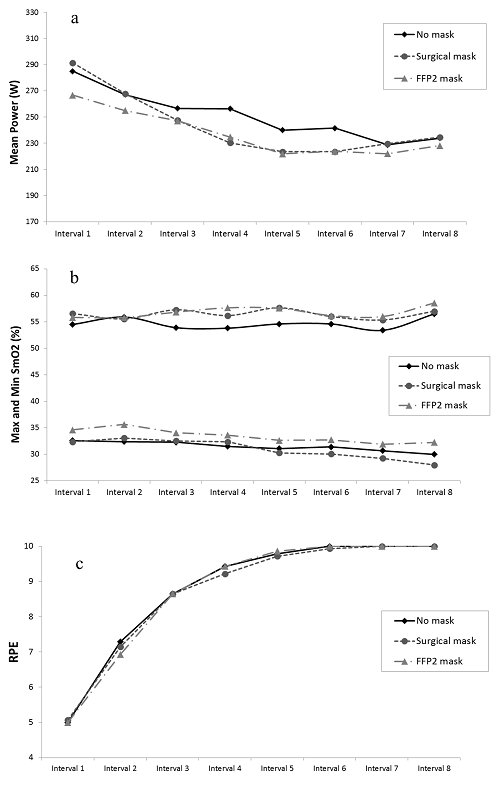
Figure 1
Mean values of cycling Power (a), SmO2 (b) and RPE (c) for each HIIT interval wearing different face masks (No, Surgical and FFP2 mask)
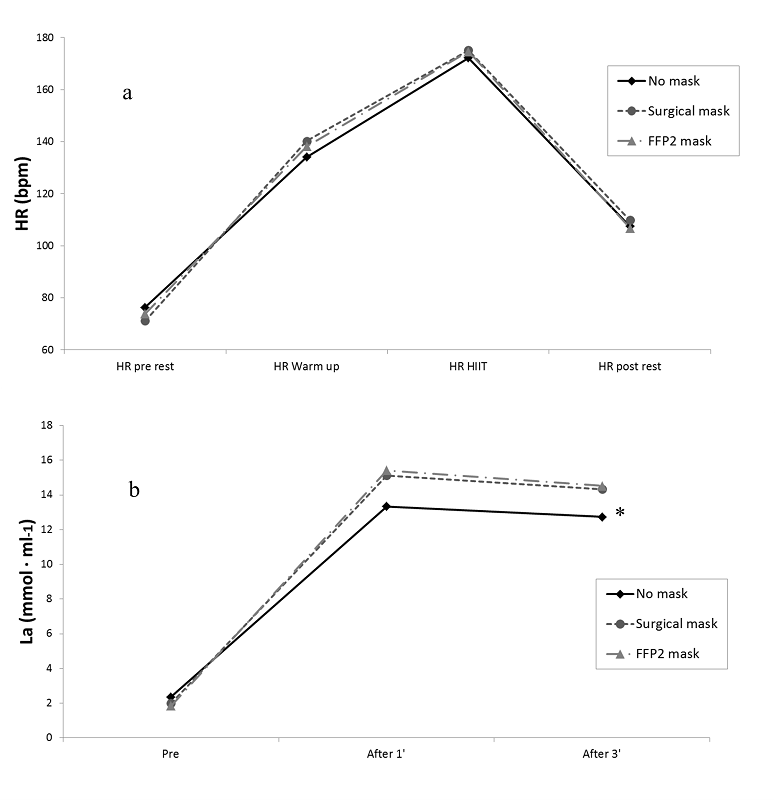
Figure 2
Mean values of HR (a) and Lactate (b) wearing different face masks (No, Surgical and FFP2 mask)
* Significant differences between No mask and FFP2 mask (p < 0.05)
Table 2 summarizes the general perception and comfort when wearing different facemasks during a HIIT protocol. Participants reported significant greater breathing difficulty, tightness, inadequacy and general discomfort when wearing the FFP2 facemask compared to the no facemask condition whereas only higher values of inadequacy and general discomfort were determined with the use of the surgical compared with no wearing facemask (p < .05).
Perception and comfort wearing different face masks (No, Surgical and FFP2 mask)
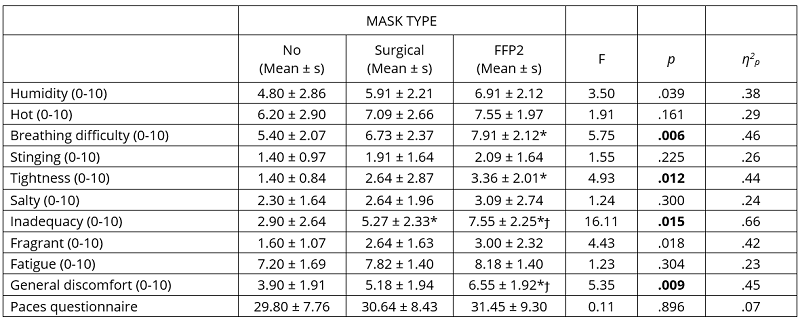
*Significant differences compared to No mask (p < 0.05)
ϯSignificant differences compared to Surgical mask (p < 0.05)
Discussion
The main finding of the current investigation was that the use of different facemask compared with not wearing facemask showed no differences in physiological parameters during the HIIT protocol. However, comfort sensation was negatively affected by the use facemask type (no mask > Surgical > FFP2).
Facemask effect on Heart Rate Variability
A factor that directly affects HRV is the practice of exercise. During exercise a variety of physiological adjustments occur to meet the demands and requirements of the body to produce energy expenditure, these adjustments result in changes due to the physiological response of the body. We have observed in our results that HRV drops drastically after the HIIT protocol. It is well known that exercise causes very significant reductions in cardiac variability (Al Haddad et al., 2010) and that exercise intensity plays a determining role on the physiological impact of the organism (Stanley et al., 2013). This must be the reason why our results show such a large impact of HIIT on HRV since it is a very high-intensity training. Although this is not a novel finding, our work shows that parasympathetic tone drops to very low levels during exercise, with this change being much greater the higher the intensity of exercise. Similarly, many studies have aimed to study how sympathetic tone behaves during and after exercise as measured by HRV. However, many studies have analyzed this fact with the use of variables such as low-frequency power (Kaikkonen et al., 2008), having recently defined that these variables are not related to sympathetic activity (Martelli et al., 2014). For this reason, in our work we have used SS to quantify sympathetic tone. We have observed that at the end of exercise, sympathetic cardiac activity increases significantly along with a very significant increase in heart rate (inverse of RR), which is one of the main effects of sympathetic activity. Therefore, it is shown how the changes provoked on HRV after exercise depend not only on a depression of sympathetic activity but also on a precursor of sympathetic tone. In fact, when analyzing the relationship between sympathetic and parasympathetic activity by means of the S/PS ratio, it is observed that the value of this variable increases significantly with HIIT. Since SS is located in the numerator and RMSSD in the denominator, an increase in S/PS values leads us to assume that the increase in post-exercise sympathetic tone is greater than parasympathetic withdrawal, showing how the sympathetic-vagal balance acts with the practice of high-intensity exercise.
The use of facemasks during intense physical exercise could compromise performance as well as cause changes in various parameters on cardiovascular markers such as the HRV. Although the HIIT interaction presented very significant values in the results shown for HRV, the mask effect showed completely opposite results. At the pre measurement, there was no difference in basal HRV before each protocol, which shows that the subjects faced the protocols with the same physiological predisposition and that the results were not affected by the change of the subjects' fitness condition. Similarly, we did not observe differences in the post results between not using a mask compared to using either mask. These results suggest that the changes in sympathovagal balance after high-intensity exercise will be the same whether or not a facemask is worn during exercise, suggesting that the use of a facemask need not negatively affect the physiological impact measured as a function of HRV.
Facemask effect on physiological parameters
Some studies argued that the use facemasks might increase resistance to inspiration and breathing (Chandrasekaran & Fernandes, 2020). The hypothesis is that air trapping in the facemask will increase rebreathing of carbon dioxide, leading to hypercapnic hypoxia as a result of increased arterial carbon dioxide due to oxygen displacement from hemoglobin (Chandrasekaran & Fernandes, 2020). However, according to the current results, no statistically significant differences were observed in muscle oxygen saturation values (SmO2). Additionally, total hemoglobin concentration at rest (THb) and during the HIIT protocol, revealed similar results than other recent investigations (Driver et al., 2021; Shaw et al., 2020).
Recent investigations found that wearing either a surgical facemask or N95 (certified filtering facepiece respirator) produces no effect on the parameters studied, but it did produce an increase in respiratory muscles during a short walk (Chen et al., 2016; Person et al., 2018). Moreover, exercising with N95 facemask was associated with a significant increase in end-tidal carbon dioxide (EtCO2) levels (Epstein et al., 2021) which could produce disturbances in respiration and consequently in general performance. Results of lactate concentrations measured 3 min after the HIIT (figure 3) showed statistically significant differences between the No facemask compared to FFP2 facemask conditions. Perhaps, the use of facemasks affects the ability of the muscle to maintain the balance between the breakdown of ATP and the production of ATP by limiting the recovery of C-reactive protein (PCr), the regulation of lactate / H + and cellular recovery after each exercise (Ramos-Campo et al., 2017). During high intensity interval training, there is a predominance of the anaerobic system and a high oxygen requirement after the cessation of activity for the conversion of the lactic acid. The use of the facemask could result in a closed circuit between oxygen and expired CO2, which could increase arterial concentrations of carbon dioxide and thus intensify the acidity of the acidic medium (Chandrasekaran & Fernandes, 2020). Although this could explain the findings of the current research, only a few studies have investigated the use of the facemask in high intensity efforts, so it would be advisable to unify methodologies for future research.
Facemask effect on perceived effort, comfort and enjoyment of physical activity
The subjective sensations as a consequence of the use of facemasks during strenuous exercise could create discomfort and consequently, a decrease in performance during exercise (Driver et al., 2021; Li et al., 2005; Scheid et al., 2020). According to the findings of the current investigation, prior research determined no significant effects of wearing a surgical or cloth facemask on RPE (Shaw et al., 2020) during a maximal cycle ergometer test. Similarly, Wong et al., (2020) found no conclusive results regarding whether wearing a facemask impairs exercise performance. In that investigation participants reported higher ratings of perceived exertion and slightly higher heart rate while exercising on a treadmill and wearing a surgical facemask compared to no-facemask condition. Additionally, during a randomized crossover design using a Bruce treadmill protocol (Driver et al., 2021) cloth facemasks led to a 14% reduction in exercise time and 29% decrease in VO2max, attributed to perceived discomfort associated with facemask-wearing. According to Azuma et al., (2018) acute respiratory acidosis can cause headache, confusion, anxiety, decreased exercise tolerance, and other possible symptoms such as fatigue, difficulty concentrating and increased heart rate and blood pressure (Redlich et al., 1997), which might be considered determining factors for the discomfort during a physical effort.
In the current investigation statistically significant differences were identified in breathing difficulty and tightness between FFP2 facemask and No facemask, as well as inadequacy and general discomfort between FFP2 facemask, the surgical and No facemask. Moreover, this cannot be due to a psychological perception, since the physical activity enjoyment questionnaire showed no significant differences with the use of any of the facemasks.
In addition, there are some aspects that may contribute to discomfort while using certain facemasks, such as size, tight elastic straps, inadequate hydration and even emotional stress caused by the pandemic (Ong et al., 2020).
An important limitation of this study was the absence of subcutaneous fat measurement in the vastus lateralis muscle, which could be a confounding factor in determining muscle oxygen saturation. Nevertheless, to ensure minimum alterations in SmO2, oxygen saturation were monitored after the placement of the device and before testing
Conclusions
The use of surgical or FFP2 facemask during a HIIT protocol did not affect oxygen saturation and performance cycling levels in physically trained women. However, perceived comfort appeared to be lower while wearing any type of facemask, especially FFP2. The findings of the present investigation have confirmed that wearing facemask did not result in a physiological barrier during strenuous exercise. Therefore, the skepticism associated with its use among athletes might be due to subjective factors. It would be advisable, for future research, to unify the methodological criteria as well as to increase the number of participants.
Bibliography
Al Haddad, H., Laursen, P. B., Ahmaidi, S., & Buchheit, M. (2010). Influence of cold water face immersion on post-exercise parasympathetic reactivation. European Journal of Applied Physiology, 108(3), 599–606. DOI: 10.1007/s00421-009-1253-9.
Azuma, Kenichi, Kagi, N., Yanagi, U., & Osawa, H. (2018). Effects of low-level inhalation exposure to carbon dioxide in indoor environments: A short review on human health and psychomotor performance. Environment International, 121, 51–56. DOI: 10.1016/j.envint.2018.08.059.
Azuma, Koichiro, & Matsumoto, H. (2016). Potential universal application of high-intensity interval training from athletes and sports lovers to patients. The Keio Journal of Medicine, 66(2), 19–24. DOI: 10.2302/kjm.2016-0006-IR.
Bailey, S. P., Willauer, T. J., Balilionis, G., Wilson, L. E., Salley, J. T., Bailey, E. K., & Strickland, T. L. (2015). Effects of an over-the-counter vented mouthguard on cardiorespiratory responses to exercise and physical agility. The Journal of Strength & Conditioning Research, 29(3), 678–684. DOI: 10.1519/JSC.0000000000000668.
Barbosa, M. P. da C. de R., Silva, A. K. F. da, Bernardo, A. F. B., Souza, N. M. de, Neto Junior, J., Pastre, C. M., & Vanderlei, L. C. M. (2014). Influence of resistance training on cardiac autonomic modulation: literature review. Medical Express. DOI: 10.5935/MedicalExpress.2014.05.13
Billat, L. V. (2001). Interval training for performance: a scientific and empirical practice. Sports Medicine, 31(1), 13–31. DOI: 10.2165/00007256-200131010-00002.
Borg, G. (1998). Borg’s perceived exertion and pain scales. Human kinetics.
Buchheit, M., & Laursen, P. B. (2013). High-intensity interval training, solutions to the programming puzzle. Sports Medicine, 43(5), 313–338. DOI: 10.1007/s40279-013-0029-x.
Camm, A., Malik, M., Bigger, J., Breithardt, G., Cerutti, S., Cohen, R., Coumel, P., Fallen, E., Kennedy, H., & Kleiger, R. E. (1996). Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation, 93(5), 1043–1065.
Chandrasekaran, B., & Fernandes, S. (2020). “Exercise with facemask; Are we handling a devil’s sword?”–A physiological hypothesis. Medical Hypotheses, 144, 110002. DOI: 10.1016/j.mehy.2020.110002.
Chen, Y., Yang, Z., Wang, J., & Gong, H. (2016). Physiological and subjective responses to breathing resistance of N95 filtering facepiece respirators in still-sitting and walking. International Journal of Industrial Ergonomics, 53, 93–101. DOI: 10.1016/j.ergon.2015.11.002.
Chu, D. K., Akl, E. A., Duda, S., Solo, K., Yaacoub, S., Schünemann, H. J., El-harakeh, A., Bognanni, A., Lotfi, T., & Loeb, M. (2020). Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. The Lancet, 395(10242), 1973–1987. DOI: 10.1016/S0140-6736(20)31142-9.
Dominelli, P. B., Molgat-Seon, Y., & Sheel, A. W. (2019). Sex differences in the pulmonary system influence the integrative response to exercise. Exercise and Sport Sciences Reviews, 47(3), 142–150. DOI: 10.1249/JES.0000000000000188.
Driver, S., Reynolds, M., Brown, K., Vingren, J. L., Hill, D. W., Bennett, M., Gilliland, T., McShan, E., Callender, L., Reynolds, E., Borunda, N., Mosolf, J., Cates, C., & Jones, A. (2022). Effects of wearing a cloth face mask on performance, physiological and perceptual responses during a graded treadmill running exercise test. British Journal of Sports Medicine, 56(2), 107-113. DOI: 10.1136/bjsports-2020-103758
Epstein, D., Korytny, A., Isenberg, Y., Marcusohn, E., Zukermann, R., Bishop, B., Minha, S., Raz, A., & Miller, A. (2021). Return to training in the COVID‐19 era: The physiological effects of face masks during exercise. Scandinavian Journal of Medicine & Science in Sports, 31(1), 70–75. DOI: 10.1111/sms.13832.
Esposito, S., Principi, N., Leung, C. C., & Migliori, G. B. (2020). Universal use of face masks for success against COVID-19: evidence and implications for prevention policies. European Respiratory Journal, 55(6). DOI: 10.1183/13993003.01260-2020.
Fikenzer, S., Uhe, T., Lavall, D., Rudolph, U., Falz, R., Busse, M., Hepp, P., & Laufs, U. (2020). Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity. Clinical Research in Cardiology, 109(12), 1522–1530. DOI: 10.1007/s00392-020-01704-y.
Gibala, M. J., Little, J. P., MacDonald, M. J., & Hawley, J. A. (2012). Physiological adaptations to low‐volume, high‐intensity interval training in health and disease. The Journal of Physiology, 590(5), 1077–1084. DOI:10.1113/jphysiol.2011.224725.
Hopkins, S. R., Dominelli, P. B., Davis, C. K., Guenette, J. A., Luks, A. M., Molgat-Seon, Y., Sá, R. C., Sheel, A. W., Swenson, E. R., & Stickland, M. K. (2021). Face masks and the cardiorespiratory response to physical activity in health and disease. Annals of the American Thoracic Society, 18(3), 399–407. DOI: 10.1513/AnnalsATS.202008-990CME.
Jacobson, T. A., Kler, J. S., Hernke, M. T., Braun, R. K., Meyer, K. C., & Funk, W. E. (2019). Direct human health risks of increased atmospheric carbon dioxide. Nature Sustainability, 2(8), 691–701. DOI: 10.1038/s41893-019-0323-1.
Kaikkonen, P., Rusko, H., & Martinmäki, K. (2008). Post‐exercise heart rate variability of endurance athletes after different high‐intensity exercise interventions. Scandinavian Journal of Medicine & Science in Sports, 18(4), 511–519. DOI: 10.1111/j.1600-0838.2007.00728.x.
Kemi, O. J., & Wisløff, U. (2010). High-intensity aerobic exercise training improves the heart in health and disease. Journal of Cardiopulmonary Rehabilitation and Prevention, 30(1), 2–11. DOI: 10.1097/HCR.0b013e3181c56b89.
Laursen, P. B., & Jenkins, D. G. (2002). The scientific basis for high-intensity interval training. Sports Medicine, 32(1), 53–73. DOI: 10.2165/00007256-200232010-00003.
Leung, N. H. L., Chu, D. K. W., Shiu, E. Y. C., Chan, K.-H., McDevitt, J. J., Hau, B. J. P., Yen, H.-L., Li, Y., Ip, D. K. M., & Peiris, J. S. M. (2020). Respiratory virus shedding in exhaled breath and efficacy of face masks. Nature Medicine, 26(5), 676–680. DOI: 10.1038/s41591-020-0843-2.
Li, Y., Tokura, H., Guo, Y. P., Wong, A. S. W., Wong, T., Chung, J., & Newton, E. (2005). Effects of wearing N95 and surgical facemasks on heart rate, thermal stress and subjective sensations. International Archives of Occupational and Environmental Health, 78(6), 501–509. DOI: 10.1007/s00420-004-0584-4.
Martelli, D., Silvani, A., McAllen, R. M., May, C. N., & Ramchandra, R. (2014). The low frequency power of heart rate variability is neither a measure of cardiac sympathetic tone nor of baroreflex sensitivity. American Journal of Physiology-Heart and Circulatory Physiology, 307(7), H1005–H1012. DOI: 10.1152/ajpheart.00361.2014
Motl, R. W., Dishman, R. K., Saunders, R., Dowda, M., Felton, G., & Pate, R. R. (2001). Measuring enjoyment of physical activity in adolescent girls. American journal of preventive medicine, 21(2), 110-117. DOI: 10.1016/s0749-3797(01)00326-9.
Moreno, J.-A., González-Cutre, D., Martínez, C., Alonso, N., & López, M. (2008). Propiedades psicométricas de la Physical Activity Enjoyment Scale (PACES) en el contexto español. Estudios de Psicología, 29(2), 173–180. DOI: 10.1174/021093908784485093.
Olcina, G., Perez-Sousa, M. Á., Escobar-Alvarez, J. A., & Timón, R. (2019). Effects of Cycling on Subsequent Running Performance, Stride Length, and Muscle Oxygen Saturation in Triathletes. Sports, 7(5), 115. DOI: 10.3390/sports7050115.
Ong, J. J. Y., Bharatendu, C., Goh, Y., Tang, J. Z. Y., Sooi, K. W. X., Tan, Y. L., Tan, B. Y. Q., Teoh, H., Ong, S. T., & Allen, D. M. (2020). Headaches associated with personal protective equipment–A cross‐sectional study among frontline healthcare workers during COVID‐19. Headache: The Journal of Head and Face Pain, 60(5), 864–877. DOI: 10.1111/head.13811.
Paquette, M., Bieuzen, F., & Billaut, F. (2020). Effect of a 3-Weeks Training Camp on Muscle Oxygenation, V˙ O2 and Performance in Elite Sprint Kayakers. Frontiers in Sports and Active Living, 2, 47. DOI: 10.3389/fspor.2020.00047.
Person, E., Lemercier, C., Royer, A., & Reychler, G. (2018). Effect of a surgical mask on six minute walking distance. Revue Des Maladies Respiratoires, 35(3), 264–268. DOI: 10.1016/j.rmr.2017.01.010.
Ramos-Campo, D. J., Rubio-Arias, J. A., Dufour, S., Chung, L., Ávila-Gandía, V., & Alcaraz, P. E. (2017). Biochemical responses and physical performance during high-intensity resistance circuit training in hypoxia and normoxia. European Journal of Applied Physiology, 117(4), 809–818. DOI: 10.1007/s00421-017-3571-7.
Redlich, C. A., Sparer, J., & Cullen, M. R. (1997). Sick-building syndrome. The Lancet, 349(9057), 1013–1016. DOI: 10.1016/S0140-6736(96)07220-0.
Scheid, J., Lupien, S., Ford, G. S., & West, S. (2020). Physiological and Psychological Impact of Face Mask Usage during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. Volume 78, Issue 18, 6655. DOI: 10.3390/ijerph17186655.
Schmitz, R. (2015). Systems and methods for measuring oxygenation. Google Patents.
Seiler, S., & Sjursen, J. E. (2004). Effect of work duration on physiological and rating scale of perceived exertion responses during self‐paced interval training. Scandinavian Journal of Medicine & Science in Sports, 14(5), 318–325. DOI: 10.1046/j.1600-0838.2003.00353.x.
Shaw, K., Butcher, S., Ko, J., Zello, G. A., & Chilibeck, P. D. (2020). Wearing of cloth or disposable surgical face masks has no effect on vigorous exercise performance in healthy individuals. International Journal of Environmental Research and Public Health, 17(21), 8110. DOI: 10.3390/ijerph17218110.
Smith, J. D., MacDougall, C. C., Johnstone, J., Copes, R. A., Schwartz, B., & Garber, G. E. (2016). Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis. Cmaj, 188(8), 567–574. DOI: 10.1503/cmaj.150835.
Stanley, J., Peake, J. M., & Buchheit, M. (2013). Cardiac parasympathetic reactivation following exercise: implications for training prescription. Sports Medicine, 43(12), 1259–1277. DOI: 10.1007/s40279-013-0083-4.
Thayer, J. F., Yamamoto, S. S., & Brosschot, J. F. (2010). The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. International Journal of Cardiology, 141(2), 122–131. DOI: 10.1016/j.ijcard.2009.09.543.
Wang, J., Pan, L., Tang, S., Ji, J. S., & Shi, X. (2020). Mask use during COVID-19: A risk adjusted strategy. Environmental Pollution, 115099. DOI: 10.1016/j.envpol.2020.115099.
Wong, A. Y.-Y., Ling, S. K.-K., Louie, L. H.-T., Law, G. Y.-K., So, R. C.-H., Lee, D. C.-W., Yau, F. C.-F., & Yung, P. S.-H. (2020). Impact of the COVID-19 pandemic on sports and exercise. Asia-Pacific Journal of Sports Medicine, Arthroscopy, Rehabilitation and Technology, 22, 39–44. DOI: 10.1016/j.asmart.2020.07.006.
Author notes
* Correspondence: Daniel López-Plaza, dlplaza@ucam.edu
Additional information
How to cite this article: Quero-Calero, C.D., López-Plaza, D., Abellán-Aynés, O., Andreu-Caravaca, L., Manonelles Marqueta, P., García-De Frutos, J.M. (2022). Acute effects of different facemasks during High Intensity Interval Training in trained women. A randomized crossover pilot study. Cultura, Ciencia y Deporte, 17(54), 15-24. https://doi.org/10.12800/ccd.v17i54.1920

ISSN: 1696-5043
Vol. 17
Num. 54
Año. 2022
Acute effects of different facemasks during High Intensity Interval Training in trained women. A randomized crossover pilot study
Carmen DanielaDanielOriolLuisPedroJosé Manuel Quero-CaleroLópez-PlazaAbellán-AynésAndreu-CaravacaManonelles MarquetaGarcía-De Frutos
International Chair of Sports Medicine, Catholic University of MurciaFaculty of Sport, Catholic University of Murcia,SpainSpain
