




Effects of active exergames training on physical functional performance in older females


Jordan Hernandez-Martínez, Rodrigo Ramirez-Campillo, Cristian Álvarez, Pablo Valdés-Badilla, Jason Moran, Mikel Izquierdo
Effects of active exergames training on physical functional performance in older females
Cultura, Ciencia y Deporte, vol. 17, no. 51, 2022
Universidad Católica San Antonio de Murcia
Jordan Hernandez-Martínez
Universidad de los Lagos., Chile
Rodrigo Ramirez-Campillo
Universidad de Los Lagos., Chile
Universidad Andres Bello., Chile
Cristian Álvarez
Universidad de Los Lagos., Chile
Pablo Valdés-Badilla * valdesbadilla@gmail.com.
Universidad Católica del Maule., Chile
Universidad Viña del Mar, Chile
Jason Moran
University Center Hartpury, Reino Unido
Mikel Izquierdo
Public University of Navarre., España
Received: 11 December 2020
Accepted: 10 November 2021
Abstract: Objective: To analyze the effects of 8 weeks of an active exergames training program on walking speed, static balance, timed up-and-go test, and sit-to-stand performance in older females. Methods: Two groups of participants were formed by block-design randomization as follows: (i) control group (n=12; age, 74.1±7.9 years); (ii) 8 week exergames training group (n=13; age, 75.6±9.1 years). Training was undertaken three times per week, including athletic, bowling and table tennis exergames. Each exergame had a duration of 8 min, with 2 min of recovery between exergames. The intensity of the training sessions was controlled using the 10-point rating of perceived exertion scale. Results: Group×time interactions were observed for the 4 m walking speed test, static balance test, timed up-and-go test and the 5-repetition sit-to-stand test (all p<0.01; d=0.46–0.80). Conclusion: Exergames training improve physical functional performance in older females. These results should be considered when designing appropriate and better training programs for older adults, since active exergames training it is an affordable and low-cost alternative for community centres and preventive health units working with this population.
Keywords: physical fitness, resistance training, frail elderly, aged, video games, exercise, musculoskeletal and neural physiological phenomena.
Resumen: Objetivo: Analizar los efectos de 8 semanas de un programa de entrenamiento de exergames activos sobre la velocidad de la marcha, el equilibrio estático, la prueba de levantarse caminar y volver a sentarse en mujeres mayores. Métodos: Se formaron dos grupos de participantes mediante aleatorización de diseño de bloques de la siguiente manera: (i) grupo de control (n = 12; edad, 74,1 ± 7,9 años); (ii) grupo de entrenamiento de exergames de 8 semanas (n = 13; edad, 75,6 ± 9,1 años). El entrenamiento se llevó a cabo tres veces por semana, incluidos ejercicios de atletismo, bolos y tenis de mesa. Cada exergame tuvo una duración de 8 min, con 2 min de recuperación entre exergames. La intensidad de las sesiones de entrenamiento se controló mediante la calificación de 10 puntos de la escala de esfuerzo percibido. Resultados: Se observaron interacciones de grupo x tiempo para la prueba de velocidad de caminata de 4 m, la prueba de equilibrio estático, la prueba de levantamiento y marcha cronometrada y la prueba de sentarse y pararse de 5 repeticiones (todas p <0,01; d = 0,46-0,80). Conclusión: El entrenamiento con exergames mejora el rendimiento físico funcional en mujeres mayores. Estos resultados deben ser considerados a la hora de diseñar programas de formación adecuados y mejores para los adultos mayores, ya que el entrenamiento en exergames es una alternativa asequible y de bajo costo para los centros comunitarios y unidades de salud preventiva que trabajan con esta población.
Palabras clave: condición física, entrenamiento de resistencia, anciano frágil, envejecido, videojuegos, ejercicio, fenómenos fisiológicos neurales y musculoesqueléticos.
INTRODUCTION
The population of older adults is increasing, with an estimated increase from 11% to 22% worldwide between years 2000 and 2050 (WHO, 2015). The aging process brings with it changes in the physical functional performance of the population, as a decrease in balance and muscle strength, leading to a deterioration in mobility, increased risk of falling, hospitalization, thus adversely affecting their quality of life and health, and may lead to functional dependence (Frontera, 2017; Smee et al., 2012).
Therefore, it is important to consider interventions to counteract the decline of physical functional performance in older adults. Physical exercise based on active exergames has emerged as a means not only of entertainment, but also as a strategy to improve the physical functional performance of older adults (Fang et al., 2020). A study by Maillot et al. (2012) demonstrated that 12 weeks of active exergames training, including two sessions per week of 70 min each, improved older males and females physical functional performance in the 6 m walk test (14%) compared to the control group (0.7%). Interventions through active exergames can offer an alternative to traditional training programs (e.g., balance training) in older adults. In a study it was observed that 6 weeks of exergames training, including five sessions of 30 min per week, improved balance (10%) and the physical functional performance in the timed up-and-go test (8.2%) in older males and females. In addition, participants reported greater pleasure during exergames training sessions compared to a group of older adults who performed traditional balance exercises (Karahan et al., 2015). In another study with older females (Szanton et al., 2016), 4 weeks (3 sessions per week) of active exergames improved balance, walking speed, and the ability to stand-up from a chair.
Furthermore, Shin et al. (2016) in an 8 week active exergames training intervention, with two sessions per week, observed improvements in the Berg balance scale (4.5%) and the timed up-and-go test (8.4%) in older males and females. In addition, improvements in the quality of life have been observed at the physical (15.1%), social (17.5%) and psychological levels (9.8%) (Keogh et al., 2012), with improvements in sociability (4.3%), decreased feelings of loneliness (6.3%) and social anxiety 2.6% (Xu et al., 2016).
While there is evidence of the favorable effects of active exergames interventions on the physical function of older adults, it is important to replicate the aforementioned findings, in order to confirm or refute results, exploring the limits of the theories and, ultimately, to help in the progression of science and society (Earp, 2015; Forstmeier et al., 2017), specially for older adults. In addition, although adequately planned active exergames interventions usually have demonstrated a significant effect on the improvement of several key outcomes in older females, the high inter-individual variability in the response to exercise training among older adults should be considered (Barbalho et al., 2017; Bouchard & Rankinen, 2001). In this sense, familial factors (shared environment and genetic factors) may affect the response to exercise training (Bouchard & Rankinen, 2001). Active exergames interventions have collected data predominantly from non-Latin-American countries, with findings potentially differencing from those that may be obtained in participants with different genetic component background (Ross et al., 2019). Therefore, the objective of this study was to replicate results previously observed in active exergames interventions in older adults from non-Latin American countries, through an 8 week active exergames training program applied to female Latin American older adults, including Amerindians (the Mapuche), to analyse its effects on physical functional performance, including walking speed, static balance, timed up-and-go test, and sit-to-stand performance. Based on relevant literature (Karahan et al., 2015; Szanton et al., 2016), it was hypothesized that 8 weeks of training with active exergames would improve the physical functional performance of older females.
METHODS
To analyze the effects of 8 weeks of an exergames training program on the physical functional performance in older females (≥60 years of age), two groups of participants were randomly formed. A block-design randomization sequence was generated electronically at https://www.randomizer.org and concealed until interventions were assigned. This procedure was established according to the “CONSORT” statement (https://www.consort-statement.org), as graphically described in Figure 1.
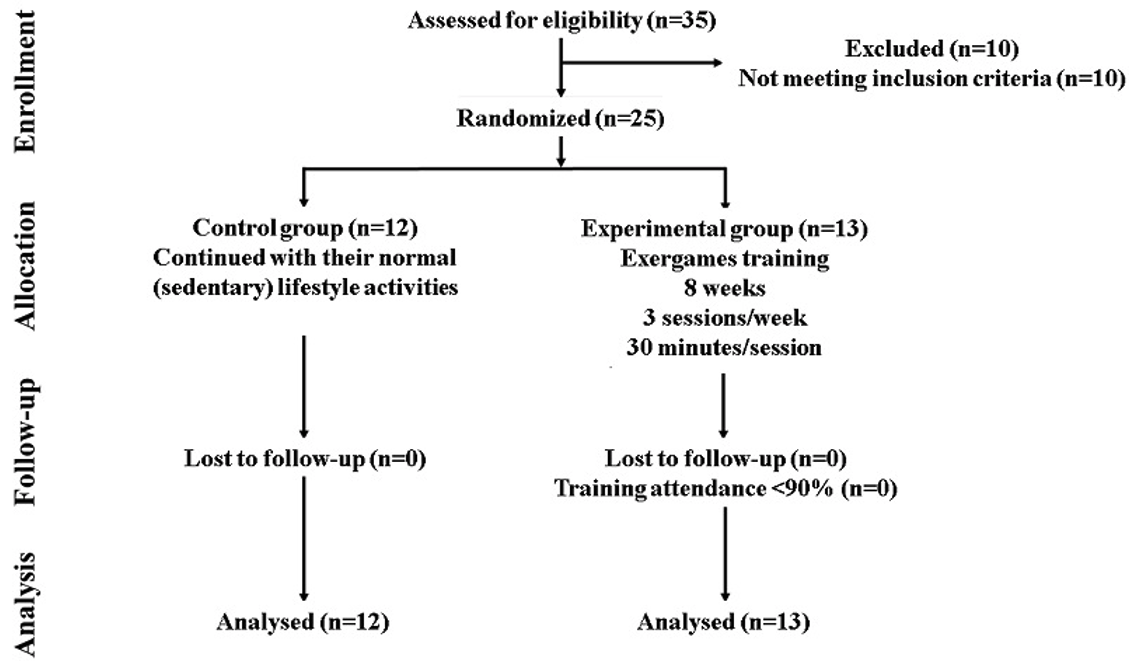
Figure 1
CONSORT diagram of recruitment and randomization process.
One group of females was deemed the control group (CG, n=12; age 74.1±7.9 years; age range, 65–89 years; body mass, 69.5±14.4 kg; height, 147.6±6.8 cm; body mass index, 31.4±5.6 kg•m-2). A second group completed 8 weeks of an active exergames training program, with three sessions per week (ExG, n=13; age, 75.6±9.1 years; age range, 60–89 years; body mass, 73.4±18.2 kg; height, 149.1±4.6 cm; body mass index, 33.1±6.7 kg•m-2).
Participants
Initially, 35 older females of Hispanic descent (including Amerindians -the Mapuche), were considered for participation in the study. Participants with similar (<600 METs-1.min-1.week-1) physical activity levels were recruited, and females from the two groups were periodically asked (i.e., three times per week) to notate their habitual physical activity levels throughout the intervention. Participants met the following inclusion criteria: (i) healthy by self-report (i.e., completion of the revised physical activity readiness questionnaire for older adults); (ii) free (by self-report) of a history of heart disease, osteoarthritis, severe visual impairment, neurological disease, pulmonary disease requiring the use of oxygen, uncontrolled hypertension, hip fracture, or lower extremity joint replacement in the past six months, and no current participation in structured training exercise or previous participation in exercise training in the past six months. Participants taking medications considered to affect dependent variables (e.g., conjugated estrogen) were excluded from the study. To be included in the final analyses, participants who met the inclusion criteria also needed to complete ≥90% of all training sessions (≥21 of 24 sessions) and attend all assessment sessions. Of the 35 females initially considered for inclusion in the study, one was excluded due to a history of heart disease, one due to a pre-existing diagnosis of osteoarthritis, and eight females did not attend all baseline measurement sessions. Therefore, 25 females were finally included and randomly divided into the CG and ExG. All females from the CG and ExG attend all measurement sessions after the intervention, and all females from the ExG attend ≥90% of all training sessions. Therefore, 25 older females were included in the final analyses. The sample size was deemed adequate for statistical power based on recommendations in previous research (Bieryla, 2016; Padala et al., 2017) examining the effects of exergames in older adults (alpha=0.05; beta=0.80).
Apart from routine daily tasks of the two groups included in the study, the ExG underwent an active exergames training program (i.e., three sessions per week over 8 weeks). All participants were carefully informed about the experimental procedures and possible risks and benefits associated with participation in the study, and each signed an informed consent document before any of the tests were performed. The study protocol was reviewed and approved by the Scientific Ethics Committee of the Universidad Autónoma de Chile (No. 06-2016) and the principles of the Declaration of Helsinki were followed for its development.
Testing procedures
Testing procedures were applied to all groups at baseline and after 8 weeks of training. The participants followed a familiarization session of 90 min before testing to reduce the effects of any differences in learning. The standardized tests were completed in one session. All tests were administered at the same location, in the same order, at the same time of day (i.e., 10:00–13:00 h), and by the same investigator, whom was blinded to the training group of the participants. Females were asked to wear the same athletic clothing during each testing session and were motivated to give their maximum effort during performance testing.
Anthropometric measures. Standing height (m) and body mass (kg) were assessed according to international standards for anthropometric assessment. To evaluate height and body mass, a stadiometer/mechanical scale (SECA, model 220, Hamburg, Germany) with accuracy of 0.1 cm and 0.1 kg, respectively, was used. These parameters were assessed before any physical performance test. Participants were tested while wearing light clothing (shoes were removed). Body mass index was calculated (kg•m-2).
4 m walking speed test. Participants were instructed to perform two maximum-effort walking for 4 m. Participants were instructed to walk as fast as possible, without running. The time was measured to the nearest 0.01 s using single-beam infrared photoelectric cells (Brower Timing System, Salt Lake City, UT, USA). Participants had a standing start with the toe of the preferred foot forward and just behind the starting line. The test started when participants voluntarily initiate the test, which triggered timing. The timing gates were positioned at the beginning (0.3 m in front of the starting line) and at 4 m and set ~0.7 m above the floor (i.e., ~hip level). This system ensures to capture trunk movement rather than a false trigger from a limb. Participants performed the trials separated by 3 min of rest, on an indoor wooden track. The best result was chosen for analysis.
Static balance. This protocol followed previous published instructions for tandem stance (Guralnik et al., 1994). An evaluator assistant was positioned on the right side of the participant, another on the left, one behind and another ahead of the participant until felt stable in the tandem position, with one foot directly in front of and touching the other foot. Participants self-selected the forward foot. Support provided was the minimum needed to prevent loss of balance and was not recorded on the data collection form or otherwise factored into the score. Timing began as support was released and continued for 10 seconds or until participants moved out of tandem or contacted external support. A stopwatch recorded the time. Two attempts were allowed and the best performance was recorded for analysis, with 2 min of rest between attempts. Instructions were given to position the arms, bend at the knees, or move the body as needed to maintain balance. The test was completed on an indoor wooden surface.
Timed up-and-go test. The test consisted of standing up from a chair (50 cm off the floor) with armrest, walking 3 m, and turning and returning to the initial seated position. The test was administered according to previously described instructions (Podsiadlo & Richardson, 1991). Participants performed three trials, with 3 min of rest between them, on an indoor wooden track. The time was measured to the nearest 0.01 s using single-beam infrared photoelectric cells (Brower Timing System, Salt Lake City, UT, USA), as indicated above. The best result was chosen for analysis.
5-repetition sit-to-stand test. The test consisted of standing up from a chair (50 cm off the floor) and returning to the initial seated position, completing five repetitions as fast as possible, administered according to previously described instructions (Guralnik et al., 1994). Time was controlled by using a stopwatch. Participants performed two trials with at least 4 min of rest between them. The best result was chosen for analysis.
Training Protocol
Training was undertaken three times per week (usually between 11:00 and 11:40), on non-consecutive days, based on previous interventions (Sadeghi et al., 2016). Exergames training sessions were conducted using an X-box® Kinect sensor containing an infrared camera that can distinguish body parts in the environment through mathematical algorithms. As the camera recognizes the joints and body parts, the avatar on the screen reflects the individual movements in real time. Participants completed the training sessions at 1.8-2.4 m in front of a big screen television, with the Kinect sensor placed ~1.5 m over the floor surface. The games selected for training sessions had three levels of intensity (difficulty): easy, moderate, and hard. In this sense, to accomplish the training principle of overload, the participants started training sessions using the easy level, increasing the difficulty according to individual progression. The intensity of the training sessions was controlled using the 10-point rating of perceived exertion (RPE) scale. However, if the training intensity was over an RPE of 4-5, the difficulty of the game was reduced. A familiarization session was held where the older females were shown how to carry out the sports games (i.e. bowling, athletics and table tennis) that would be included in their exergames training. After this, he was asked if there was any doubt to explain again. Continuing with older adults playing these games in a recreational way so they can adapt to this technology.
Training sessions begun with a warm-up of 5 min, including a lateral step to the right and then to the left, four times in each direction, walking forward and energetically, raising the left and right knee upwards, and mild stretching. The main part of the training sessions included athletic, bowling and table tennis exergames, each with a duration of 8 min, with 2 min of recovery between games. All training sessions finished with a cool-down of 5 min, including breathing deeply while carrying both arms above the head and letting out the air while bringing the arms back down, walking slowly, and performing some mild stretching exercises (Sadeghi et al., 2016). Training sessions were performed under the direct supervision of strength and conditioning coaches to ensure safety and the maintenance of the exercise protocol. A supervisor-to-participant ratio method of 1:1 was used. The strength and conditioning coaches were oriented to: (i) control training attendance and administration (i.e., check participants’ training logs after each training session and help them to complete the logs); (ii) provide technical instruction, feedback, and motivation to assure adequate training intensity; (iii) provide social and mental support; and (iv) exhibit a supportive attitude and avoid over-expectation. None of the coaches was aware of the purpose of the study. On the other hand, intensity was increased in table tennis and athletics games by growing the speed of movements, while for bowling, the game's complexity was increased. Figure 2 presents the summary of the intervention.
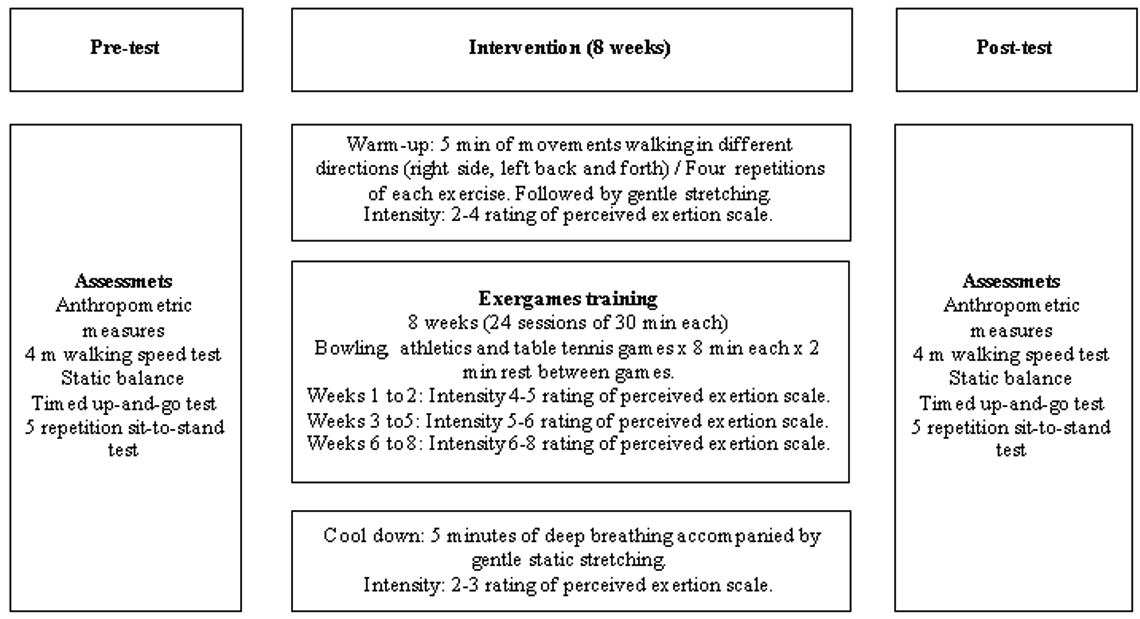
Figure 2
Intervention program
Statistical analysis
Data are presented as group mean values ± standard deviations. Normality and homoscedasticity assumptions for all data before and after intervention were checked with Shapiro-Wilk and Levene tests, respectively. Differences between groups at baseline were investigated using one-way ANOVA test. To establish the effects of the intervention on the outcomes, ANOVA with repeated measures (two groups [Control and Experimental] × two time points [pre- and post- test]) were performed. Post-hoc tests with a Bonferroni-adjusted α were conducted to identify comparisons that were statistically significant. Effect sizes for main effects of group, time, as well as group × time interactions were taken from the ANOVA output (partial eta squared). Within-group Cohen’s d effect sizes were computed, using the following equation: effect sizes = (mean_post - mean_pre)/pooled standard deviation. Statistical analyses were conducted using STATISTICA statistical package (Version 8.0; StatSoft, Inc, Tulsa). Significance level was set at α = 5%. Tests’ reliability was determined using the intra-class correlation coefficient, with threshold set at ≥0.80 in order to include data for analysis.
RESULTS
No injuries occurred in any of the females during the completion of this study. Moreover, although participants described mild levels of muscle soreness after the initial testing and training sessions, none of them suspended training or their normal daily live activities due to muscle soreness.
There were no significant (all p>0.05, d=0.01–0.11) baseline differences between-groups for all dependent variables (Table 1).
Baseline pre and changes post in dependent variables after 8 weeks of intervention
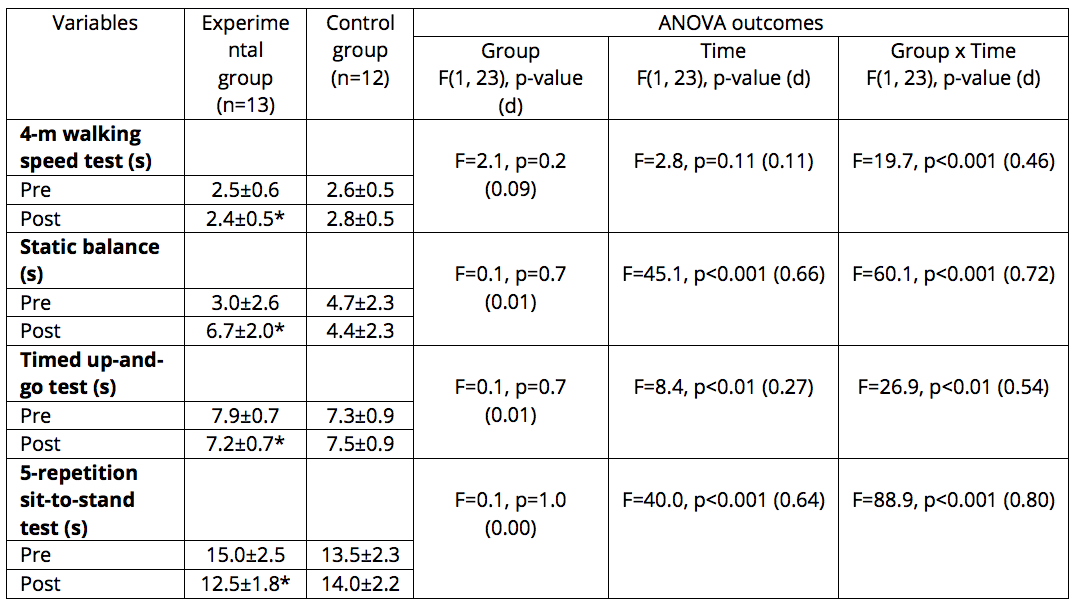
Group × time interactions were observed for the 4 m walking speed test, static balance, timed up-and-go test, and 5-repetition sit-to-stand test (all p<0.01; d=0.46–0.80). For the ExG, the improvements in the 4 m walking speed test was Δ4.1% (d=0.22), static balance Δ199% (d=1.42), timed up-and-go test Δ8.5% (d=0.85), and 5-repetition sit-to-stand test Δ16% (d=1.07). Aside from trivial (ES <0.2) changes in the CG for the static balance, timed up-and-go test, and 5-repetition sit-to-stand test, a detrimental change was detected in the 4 m walking speed test after 8 weeks (Δ10.9%, d=0.5).
DISCUSSION
The objective of this study was to replicate results previously observed in active exergames interventions in older adults from non-Latin-American countries, through an 8 week active exergames training program applied to female Latin American older adults, including Amerindians (the Mapuche), to analyze its effects on walking speed, static balance, timed up-and-go test, and sit-to-stand performance. The main results suggest that an 8-week active exergames training program induced meaningful improvements in the 4 m walking speed test, static balance, timed up-and-go test, and 5-repetition sit-to-stand test, as compared to a control group.
Walking is an essential part of daily living, and even a performance increase of 0.1 m.s-1 in walking speed has been associated with increased survival, especially in older females (Studenski et al., 2011). Additionally, improvements in this physical capability may reduce the difficulty with which older females perform their daily living activities, giving them the possibility of better walking habits and, hence, improved health (Mosallanezhad et al., 2013). In this sense, current results show that the ExG, after an exergames training program intervention, improved in the 4 m walking speed test (d=0.22), similar to previous exergames training interventions in older females. According to Garcia et al. (2016) improvements in walking speed (29%) were observed after an intervention with twelve weeks and three sessions per week in older females and males. Szanton et al. (2016), after a 4-week intervention, with three sessions per week, induced a 19.4% improvement in walking speed in older adults. Improvements may be associated with greater neuromuscular activation and muscle power (Clark et al., 2011; Suzuki et al., 2001).
Alterations in the proprioceptive, sensory and vestibular systems occur frequently during aging (Clark et al., 2015), leading to a loss of control of the knee joint and balance (Relph & Herrington, 2016). Such changes may be counteracted by appropriate interventions. In this sense, current results show that the ExG, after an exergames training program, improved in the static balance test (d=1.42). Similar to the current results, Karahan et al. (2015) after 6 weeks and 5 sessions per week, observed improvements (10.2%) in the Berg balance scale in older adults. Changes in balance after exergames training might be related to an improvement in the proprioception of the knee joint (Sadeghi et al., 2016). After 8 weeks of exergames training, with 3 sessions per week (as in the current study), an improvement in knee proprioception was observed in the dominant and non-dominant leg in older participants (Sadeghi et al., 2016). Exergames training programs combines sensory stimulation with cognitive stimulation (Saposnik et al., 2009) including multisensory feedback (Pichierri et al., 2011) which may be related to the aforementioned proprioception and balance improvement. Therefore, to counteract the falls during aging due to poor proprioception and postural stability (Sohn & Kim, 2015) the sensorial motor-control stimulation induced by exergames training, especially in the lower-limbs, may be important for balance.
Limitations in the mobility of the lower limbs, such as walking or getting up from a chair are also indicators of a marked decline in functional health (Verbrugge & Jette, 1994). In this sense, a key finding in this study was the improvement in the timed up-and-go test (Δ8.5%, d=0.85) in the ExG, corroborating previous results. For example, after 12 weeks of exergames training, with 3 sessions per week, improvements (13%) were observed in the timed up-and-go test in older adults (Garcia et al., 2016). In addition, Grigorova et al. (2015) observed improvements (6.8%) in the timed up-and-go test after 4 weeks. Interventions with exergames may lead to an increase in the strength of the lower limbs and balance, potentially related to improvements in the timed up-and-go test (Grigorova et al., 2015; Lee, 2013). Such adaptations may lead to decreased fear and risk of falling.
Improvements in the 5-repetition sit-to-stand test (Δ16%, d=1.07) was also observed in this study. Similarly, Sato et al. (2015) after 24 active exergames training sessions, observed improvements (37.1%) in standing and sitting from a chair in older adults. As some of the games included in the current intervention required that participants perform movements similar to the sit-to-stand test, this may have contributed to the observed changes in physical functional performance. For example, during bowling, table-tennis and the long jump in athletics exergames the participants frequently adopted a ~90° knee angle, similar to the knee angle that may be considered key for the performance of the sit-to-stand test. In this line, a previous study in older adults also observed improvements in the sit-to-stand test after an exergames intervention that included games with a similar pattern of movement (Sato et al., 2015). Improvements in the sit-to-stand test may be considered key for the physical autonomy of older adults to carry out their activities of daily living.
A possible limitation of the present study was the absence of more physiological measurements, which may have helped in better understanding the underlying mechanisms of active exergames training. Moreover, further studies should aim to replicate current results with greater samples sizes of older females, and older males, including long-term assessments. Despite of these limitations, this study provides support for using active exergames training as an accessible alternative to promote active aging.
CONCLUSION
An 8-week active exergames training program induced meaningful improvements in the physical functional performance of older females, including improvements in the 4 m walking speed test, static balance, timed up-and-go test, and the 5-repetition sit-to-stand test, as compared to a control group of females that continued with their habitual non-active lifestyle.
PRACTICAL APPLICATIONS
Active exergames training approaches may be an effective and safe strategy to achieve significant and clinically relevant improvements in physical functional performance relevant to activities of daily living and the quality of life of older females. These results should be considered when designing appropriate and better training programs for older adults, since active exergames training it is an affordable and low-cost alternative for community centers and preventive health units working with this population.
Financing
No financial support received by the authors.
REFERENCES
Barbalho, M., Gentil, P., Izquierdo, M., Fisher, J., Steele, J., & Raiol, RA. (2017). There are no no-responders to low or high resistance training volumes among older women. Experimental Gerontology, 99:18-26. doi: 10.1016/j.exger.2017.09.003.
Bieryla, KA. (2016). Xbox Kinect training to improve clinical measures of balance in older adults: a pilot study. Aging Clinical and Experimental Research, 28(3):451-7. doi: 10.1007/s40520-015-0452-y.
Bouchard, C., & Rankinen, T. (2001). Individual differences in response to regular physical activity. Medicine & Science in Sports and Exercise, 33(6):S446-51. doi: 10.1097/00005768-200106001-00013
Clark, D.J., Patten, C., Reid, K.F., Carabello, R.J., Phillips, E.M., & Fielding, R.A. (2011). Muscle performance and physical function are associated with voluntary rate of neuromuscular activation in older adults. The Journal of Gerontology. Series A, Biological Science and Medical Sciences, 66(1):115-21. doi: 10.1093/gerona/glq153
Clark, N.C., Roijezon, U., & Treleaven, J. (2015). Proprioception in musculoskeletal rehabilitation. Part 2: Clinical assessment and intervention. Manual Therapy, 20(3):378-87. doi: 10.1016/j.math.2015.01.009.
Earp, B.D., & Trafimow, D. (2015). Replication, falsification, and the crisis of confidence in social psychology. Frontiers in Psychology, 6: 621. doi: 10.3389/fpsyg.2015.00621
Fang, Q., Ghanouni, P., Anderson, S.E., Touchett, H., Shirley, R., Fang, F., & Fang, C. (2020). Effects of exergaming on balance of healthy older adults: a systematic review and meta-analysis of randomized controlled trials. Games for health journal, 9(1), 11-23. doi: 10.1089/g4h.2019.0016.
Forstmeier. W., Wagenmakers, E.J., & Parker, T.H. (2017). Detecting and avoiding likely false-positive findings - a practical guide. Biological Reviews, 92(4):1941-1968. doi: 10.1111/brv.12315.
Frontera, W.R. (2017). Physiologic Changes of the Musculoskeletal System with Aging: A Brief Review. Physical Medicine and Rehabilitation Clinics of North America, 28(4):705-711. doi:10.1016/j.pmr.2017.06.004.
Garcia, J.A., Schoene, D., Lord, SR., Delbaere, K., Valenzuela, T., & Navarro, K.F. (2016). A Bespoke Kinect Stepping Exergame for Improving Physical and Cognitive Function in Older People: A Pilot Study. Games for Health Journal, 5(6), 382–388. doi: 10.1089/g4h.2016.0070
Grigorova, K, Dimitrova, A, Lubenova, D, Zaharieva, D., & Vasileva, D. (2015). Feasibility of interactive video games for influence on balance in institutionalized elderly people. Journal of Physical Education and Sport, 15(31): 429-43. doi: 10.7752/jpes.2015.03064.h
Guralnik, J.M., Simonsick, E.M., Ferrucci, L., Glynn, R.J., Berkman, L.F., Blazer, D.G., Scherr, P.A., & Wallace R.B. (1994). A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. Journal Gerontology, 49(2):M85-94. doi: 10.1093/geronj/49.2.m85.
Karahan AY., Tok F., Taskin H., Kucuksarac S., Basaran A., & Yildirim P. (2015). Effects of Exergames on Balance, Functional Mobility, and Quality of Life of Geriatrics Versus Home Exercise Programme: Randomized Controlled Study. Central European Journal of Public Health, 23 Suppl:S14-8. doi: 10.21101/cejph.a4081.
Keogh, J.W., Power, N., Wooller, L., Lucas, P., & Whatman, C. (2014). Physical and psychosocial function in residential aged-care elders: effect of Nintendo Wii Sports games. Journal of Aging Physical Activity, 22(2):235-44. doi: 10.1123/japa.2012-0272.
Lee, G. (2013). Effects of training using video games on the muscle strength, muscle tone, and activities of daily living of chronic stroke patients. Journal of Physical Therapy Science, 25(5): 595–597. doi: 10.1589/jpts.25.595.
Maillot, P., Perrot, A., & Hartley, A. (2012). Effects of interactive physical-activity video-game training on physical and cognitive function in older adults. Psychology and Aging, 27(3):589-600. doi: 10.1037/a0026268.
Mosallanezhad, Z., Salavati, M., Sotoudeh, G.R., Nilsson W.L., & Frandin, K. (2014). Walking habits and health-related factors in 75-year-old Iranian women and men. Archives of Gerontology and Geriatrics, 58(3):320-6. doi: 10.1016/j.archger.2013.11.008.
Padala, K.P., Padala, P.R., Lensing, S.Y., Dennis, R.A., Bopp, M.M., Parkes, C.M., Garrison M.K., Dubbert, P.M., Roberson, P.K., & Sullivan, D.H. (2017). Efficacy of Wii-Fit on Static and Dynamic Balance in Community Dwelling Older Veterans: A Randomized Controlled Pilot Trial. Journal of Aging Research, 4653635. doi: 10.1155/2017/4653635.
Pichierri, G., Wolf, P., Murer, K., & de Bruin, E.D. (2011). Cognitive and cognitive-motor interventions affecting physical functioning: a systematic review. BMC Geriatrics, 11-29. doi:10.1186/1471-2318-11-29.
Podsiadlo, D., & Richardson, S. (1991). The timed "Up & Go": a test of basic functional mobility for frail elderly persons. Journal of the American Geriatrics Society, 39(2):142-8. doi: 10.1111/j.1532-5415.1991.tb01616.x.
Relph, N., & Herrington, L. (2016). The effects of knee direction, physical activity and age on knee joint position sense. The Knee, 23(3):393-8. doi: 10.1016/j.knee.2016.02.018.
Ross, R., Goodpaster, B.H., Koch, L.G., Sarzynski, M.A., Kohrt, W.M., Johannsen, N.M., Skinner, J.S., Castro, A., Irving, B.A., Noland, R.C., Sparks, L.M., Spielmann, G., Day, A.G., Pitsch, W., Hopkins, W.G., & Bouchard, C. (2019). Precision exercise medicine: understanding exercise response variability. British Journal of Sports Medicine, 53(18):1141-1153. doi: 10.1136/bjsports-2018-100328.
Sadeghi, H., Hakim, M.N., Hamid, T.A., Amri, S.B., Razeghi, M., Farazdaghi, M., & Shakoor, E. (2017). The effect of exergaming on knee proprioception in older men: A randomized controlled trial. Archives of Gerontology and Geriatrics 2017, 69:144-150. doi: 10.1016/j.archger.2016.11.009.
Saposnik, G., Mamdani, M., Bayley, M., Thorpe, K.E., Hall, J., Cohen, L.G., & Teasell, R. (2010). Effectiveness of Virtual Reality Exercises in STroke Rehabilitation (EVREST): rationale, design, and protocol of a pilot randomized clinical trial assessing the Wii gaming system. International Journal of Stroke, 5(1):47-51. doi: 10.1111/j.1747-4949.2009.00404.x.
Sato, K., Kuroki, K., Saiki, S., & Nagatomi, R. (2015). Improving Walking, Muscle Strength, and Balance in the Elderly with an Exergame Using Kinect: A Randomized Controlled Trial. Randomized Controlled Trial. Games for Health Journal, 4(3):161-7. doi: 10.1089/g4h.2014.0057.
Shih, M.C., Wang, R.Y., Cheng, S.J., & Yang, Y.R. (2016). Effects of a balance-based exergaming intervention using the Kinect sensor on posture stability in individuals with Parkinson's disease: a single-blinded randomized controlled trial. Journal Neuroengineering and Rehabilitation, 27:13(1):78. doi: 10.1186/s12984-016-0185-y.
Smee, D.J., Anson, J.M., Waddington, G.S., & Berry, H.L. (2012). Association between Physical Functionality and Falls Risk in Community-Living Older Adults. Current Gerontology and Geriatrics Research, 864516. doi: 10.1155/2012/864516
Sohn, J., & Kim, S. (2015). Falls study: Proprioception, postural stability, and slips. Biomedical Materials and Engineering, 26 Suppl 1:S693-703. doi: 10.3233/BME-151361.
Studenski, S., Perera, S., Patel, K., Rosano, C., Faulkner, K., Inzitari, M., Brach, J., Chandler, J., Cawthon, P., Connor, E.B., Nevitt, M., Visser, M., Kritchevsky, S., Badinelli, S., Harris, T., Newman, A.B., Cauley, J., Ferrucci, L., & Guralnik, J. (2011). Gait speed and survival in older adults. JAMA, 305(1): 50–58. doi: 10.1001/jama.2010.1923.
Suzuki, T., Bean, J.F., & Fielding, R.A. (2001). Muscle power of the ankle flexors predicts functional performance in community-dwelling older women. Journal of the American Geriatrics Society, 49(9):1161-7. doi: 10.1046/j.1532-5415.2001.49232.x.
Szanton, SL., Walker, R.K., Lim, J.H., Fisher, L., Zhan, A., Gitlin, L.N., Thorpe, R.J., & Terzis, A. (2016). Development of an Exergame for Urban-dwelling Older Adults With Functional Limitations: Results and Lessons Learned. Progress in community health partnerships: research, education, and action, 10(1):73-81. doi: 10.1353/cpr.2016.0005.
Verbrugge, L.M., & Jette, A.M. (1994). The disablement process. Social science & medicine, 38(1):1-14. doi: 10.1016/0277-9536(94)90294-1.
WHO (World Health Organization). World report on ageing and health. World Health Organization, ed.: World Health Organization, 2015. URL: https://apps.who.int/iris/handle/10665/186463.
Xu, X., Li, J., Pham, T.P., Salmon, C.T., & Theng, Y.L. (2016). Improving Psychosocial Well-Being of Older Adults Through Exergaming: The Moderation Effects of Intergenerational Communication and Age Cohorts. Games for health journal, 5 (6):389-397. https://doi.org/10.1089/g4h.2016.0060.
Author notes
* Autor para la correspondencia. Teléfono: +56 9 71258824. Email: valdesbadilla@gmail.com
Additional information
HOW TO CITE: Hernandez-Martínez, J., Ramirez-Campillo, R., Álvarez, C., Valdés-Badilla, P., Moran, J., Izquierdo, M. (2022). Effects of active exergames training on physical functional performance in older females. Cultura, Ciencia y Deporte.

ISSN: 1696-5043
Vol. 17
Num. 51
Año. 2022
Effects of active exergames training on physical functional performance in older females
JordanRodrigoCristianPabloJasonMikel Hernandez-MartínezRamirez-CampilloÁlvarezValdés-BadillaMoranIzquierdo
Universidad de los Lagos.Universidad de Los Lagos.Universidad Andres Bello.Universidad de Los Lagos.Universidad Católica del Maule.Universidad Viña del MarUniversity Center HartpuryPublic University of Navarre.,ChileChileChileChileChileChileReino UnidoEspaña
